Corewell Health William Beaumont University Hospital Royal Oak, MI
Muhammad Ibrahim Majeed, MD1, Samiksha Pandey, MD1, Mehr Amer Majeed, MD2, Usman Bin Hameed, MD1, Wael Dahhan, MD1 1Corewell Health William Beaumont University Hospital, Royal Oak, MI; 2SSM Health Saint Louis University Hospital, St. Louis, MO Introduction: Breast carcinoma is the most common malignancy in women and the leading cause of cancer-related deaths in this population. Common metastatic sites include lymph nodes, bone, lungs, liver, and brain. However, gastric metastases are rare. We present a case of newly diagnosed metastatic breast cancer identified through gastric ulcer biopsy.
Case Description/
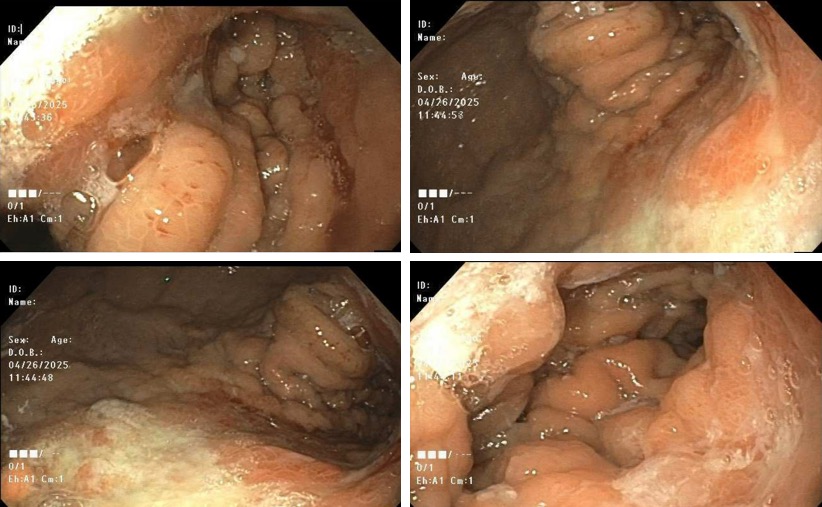
Methods: A 74-year-old female with nonischemic cardiomyopathy, and prior cardiac arrest with an implantable cardioverter-defibrillator (ICD) presented with a two-month history of dyspepsia, epigastric pain, anorexia and 40-pound unintentional weight loss. She denied fever, nausea, vomiting, melena or hematochezia and had a benign abdominal exam. Laboratory studies showed hemoglobin 11.8 g/dL, ALP 112 U/L, AST 18 U/L, ALT 5 U/L, and lipase 11 U/L. Abdominal ultrasound revealed persistent circumferential distal gastric wall thickening, which was also seen on Computed Tomography (CT) Abdomen, one month earlier. Esophageogastroduodenoscopy (EGD) showed severe edematous, erythematous and ulcerated mucosa in the body and antrum of the stomach without active bleeding (figure 1), consistent with gastritis and suspicious for malignancy. Gastric biopsies revealed infiltrating metastatic hormone receptor-positive, HER2-low breast carcinoma. Notably, the patient had not been compliant with her screening mammograms. CT head did not reveal intracranial metastases but did show osseous lesions suggestive of bone metastases. The patient was started on letrozole, with plans for further workup and initiation of concomitant cyclin-dependent kinase 4/6 inhibitor and denosumab outpatient. She was not a candidate for radiation therapy due to presence of an ICD. Discussion: This case highlights the rarity of gastric metastases and the critical role of a thorough gastrointestinal (GI) evaluation in uncovering an underlying malignancy. To our knowledge, this is the only reported case where primary breast cancer was first identified through GI symptoms and confirmed by gastric biopsy. Clinicians should therefore, maintain a high index of suspicion for metastatic disease in female patients presenting with red flag symptoms, such as significant weight loss in the context of nonspecific GI complaints. This case also emphasizes the importance of adherence to screening protocols, such as mammography, which are essential for early detection and treatment of potentially aggressive breast cancers.
Figure: Figure 1: Endoscopic images of gastric mucosa showing inflammation, friability and ulcer.
Disclosures: Muhammad Ibrahim Majeed indicated no relevant financial relationships. Samiksha Pandey indicated no relevant financial relationships. Mehr Amer Majeed indicated no relevant financial relationships. Usman Bin Hameed indicated no relevant financial relationships. Wael Dahhan indicated no relevant financial relationships.
Muhammad Ibrahim Majeed, MD1, Samiksha Pandey, MD1, Mehr Amer Majeed, MD2, Usman Bin Hameed, MD1, Wael Dahhan, MD1. P6418 - Silent Until the Stomach Spoke: Breast Cancer Discovered Through Gastric Metastasis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")