Bilal Niazi, MD1, Derrick Antoniak, MD2, Rebecca Romero, PA3, Maura O'Neil, MD3 1University of Nebraska Medical Center, Omaha, NE; 2Department of Gastroenterology, University of Nebraska Medical Center; Department of Veterans Affairs, Nebraska-Western Iowa Healthcare System, Omaha, NE; 3University of Kansas Medical Center, Kansas City, KS Introduction: CDH1 associated gastric cancer is a unique diffuse-type, signet ring cell gastric cancer. Carriers of the pathogenic CDH1 gene carry an estimated lifetime gastric cancer risk up to 83%. Due to the disruption of cell adhesion complex, these cancers are poorly adhesive and diffusely infiltrating. This makes them difficult to diagnose endoscopically, with symptoms often arising late in the disease course.
Idiopathic gastroparesis (GP) is a variant of GP that is most often low grade, fluctuating in severity, and typically presents in young or middle-age females with underlying psychiatric comorbidities and overlapping functional gastrointestinal conditions.
Here we present the case of a previously healthy male who was diagnosed with idiopathic grade 4 GP and later found to have CDH1 gastric cancer with metastasis. To the best of our knowledge, this is the first documented case of CDH1 associated gastric cancer presenting as gastroparesis.
Case Description/
Methods: A 44-year-old male with no medical history presented with persistent nausea, vomiting, and early satiety. Initial workup included upper and lower endoscopy, imaging, and gastric emptying study (GES). Upper endoscopy described gastric erythema, congested antral mucosa, and prepyloric narrowing. Colonoscopy and initial imaging were unremarkable. GES revealed 82% retention at 4 hours. The patient was given a diagnosis of idiopathic GP and trialed on pro-motility agents with minimal relief.
Due to ongoing symptoms, 100-pound weight loss, and severe malnutrition, he presented to our facility for evaluation. Labs were unremarkable apart from signs of poor nutrition, and CT scan showed severe gastric distention. Post-pyloric access was obtained, and he was started on tube feeds. During discussion, he revealed a family history of gastric and breast cancer as well as a pathogenic CDH1 mutation. Genetic counseling and testing were performed, and after his testing returned positive for a pathogenic CDH1 allele, he was referred for gastrectomy. At the time of surgery, he was found to have diffuse gastric cancer and serosal metastases. Discussion: CDH1-associated gastric cancer is often indolent and difficult to diagnose endoscopically. Delay in diagnosis can have devastating impacts including metastatic spread as seen in our patient. GP is not a known presentation of CDH1 gastric cancer. In presenting our case we hope to bring awareness of GP as a potential early sign of CDH1-associated gastric cancer.
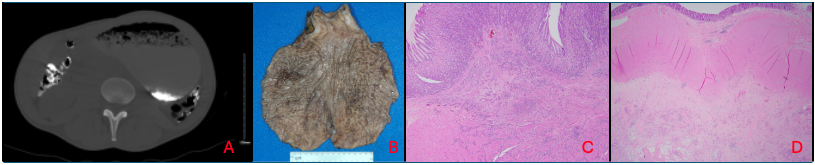
Figure: Figure 1: Displayed here are the CT imaging, gross specimen, and pathology from the stomach and transverse colon. In slide A, the CT reveals significant distention of the abdomen with retained contents. Slide B reveals a gross specimen of the stomach, without any obvious macroscopic abnormalities. Slide C reveals discohesive malignant cells infiltrating the mucosa, submucosa, and muscularis propria of the gastrectomy specimen. Slide D reveals discohesive malignant cells infiltrating the serosa and muscularis propria of the transverse colon.
Disclosures: Bilal Niazi indicated no relevant financial relationships. Derrick Antoniak indicated no relevant financial relationships. Rebecca Romero indicated no relevant financial relationships. Maura O'Neil indicated no relevant financial relationships.
Bilal Niazi, MD1, Derrick Antoniak, MD2, Rebecca Romero, PA3, Maura O'Neil, MD3. P6412 - CDH1-Associated Gastric Cancer Masquerading as Gastroparesis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")