Allegheny Health Network Medicine Institute Pittsburgh, PA
Helene Bloom, DO1, Alexandra M. Johnston, DO2, Marissa Gorvet, DO1 1Allegheny Health Network Medicine Institute, Pittsburgh, PA; 2Allegheny Health Network, Pittsburgh, PA Introduction: In rare cases, gastric ulcerations can create a fistulous tract between the pre-pyloric stomach and duodenal bulb, resulting in a “double pylorus”. A double pylorus is seen in up to 0.4% of endoscopies and results from either a congenital or acquired deformity within the distal stomach. Risk factors include H. Pylori infection, diabetes and NSAID use. We present a rare case of double pylorus secondary to a gastric ulcer in an elderly female presenting with ongoing abdominal bloating, vomiting, and weight loss.
Case Description/
Methods: A 68-year-old female with a past history of hypertension, hyperlipidemia, osteoarthritis with intermittent Ibuprofen use and OSA on CPAP presented with a new onset of abdominal bloating, vomiting, decreased appetite, and a 5-pound weight loss. She had a recent change in her CPAP settings and felt this was attributing to her symptoms. She began taking as-needed Pepcid and Protonix and decreased her CPAP usage with improvement. Therefore, she declined further evaluation with EGD and it was recommended that she increase her Protonix to 40 mg daily. She re-presented three months later with worsening symptoms including right upper quadrant abdominal pain, and an 11-pound weight loss. CT abdomen and pelvis with contrast was remarkable for a small hiatal hernia. EGD showed a 10 mm cratered pre-pyloric gastric ulcer. The ulcer perforated the stomach creating a fistula between the pylorus and duodenal bulb. Her Protonix was further increased to 40 mg twice daily. Biopsies were negative for H. pylori. On repeat EGD, there was a persistent medium-sized fistula in the pre-pyloric region of the stomach with communication to the duodenum and two localized non-bleeding erosions in the pre-pyloric region at the site of the fistula. The prior ulcerated area appeared mostly healed. Her Protonix was decreased to 40 mg daily for three months followed by 20 mg daily with full resolution of symptoms. Discussion: Although rare, a double pylorus can be acquired from chronic peptic ulcer disease commonly caused by an H. pylori infection or NSAID use. It is important to complete further endoscopic workup in patients with red flag symptoms and provide comprehensive education on symptomatology associated with possible diagnoses and appropriate diagnostic testing when patients are hesitant to invasive interventions. In this case doing so ultimately led to the discovery of pre-pyloric gastric ulceration with a rare finding of gastroduodenal fistula creating a double pylorus.
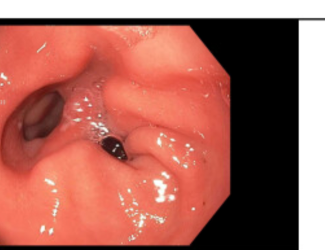
Figure: Image 1: Initial endoscopy with 10 mm cratered pre-pyloric ulcer and gastroduodenal fistula
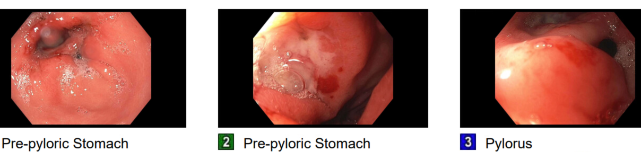
Figure: Image 2: Three month follow-up endoscopy showcasing healed gastric ulcer and double pylorus
Disclosures: Helene Bloom indicated no relevant financial relationships. Alexandra Johnston indicated no relevant financial relationships. Marissa Gorvet indicated no relevant financial relationships.
Helene Bloom, DO1, Alexandra M. Johnston, DO2, Marissa Gorvet, DO1. P6363 - Double Trouble: A Case of Double Pylorus Secondary to a Pre-Pyloric Gastric Ulcer, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.