Angelin Raju, MD1, Anish Jomy, MBBS2, Gaurav Arora, MD3, James Nackley, MD1, Anunaya Aashish, MD1, Ashni Dudhia, DO1, Daniel Gonzalez, MD1, Maher Taha, MD4, Amna Naveed Butt, MD5 1Texas Health Resources HEB/ Denton, Bedford, TX; 2Methodist Health System, Richardson, TX; 3Texas Health Presbyterian Hospital Denton, Denton, TX; 4Texas Health Resources, Irving, TX; 5Texas Health Resources, Haslet, TX Introduction: Gastric diverticula (GD) are the rarest form of gastrointestinal tract diverticulumwith an estimated incidence of 0.013–2.6% and extremely low rate of bleeding. While most are asymptomatic and discovered incidentally, complications such as life-threatening bleeding, perforation can occur, though they are exceedingly rare. Upper gastrointestinal (GI) bleeding from a gastric diverticulum is a seldom-reported phenomenon, with only a handful of documented cases in the literature. We present a case of a 71-year-old female with hematemesis secondary to bleeding from a gastric fundus diverticulum, successfully managed with endoscopic therapy. This case highlights the importance of considering gastric diverticula in the differential diagnosis of obscure upper GI bleeding, particularly when more common etiologies (e.g., peptic ulcers, varices, Mallory-Weiss tears) have been excluded.
Case Description/
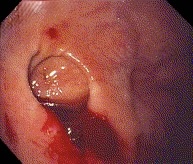
Methods: 71-year-old white female with multiple comorbidities including GERD, dysphagia, irritable bowel syndrome presented with acute nausea, vomiting, and hematemesis. Initial hemoglobin was 10.9 g/dL which dropped to 8.5 g/dL. CT abdomen/pelvis with contrast was unremarkable except for a stable splenic artery aneurysm. EGD revealed a 2 cm actively bleeding diverticulum in the proximal gastric fundus, which was treated with epinephrine injection, 8 hemoclips, and Hemospray. Large fresh blood/clots were evacuated via Roth net. No further hematemesis or bleeding was observed post-intervention. The diverticular bleed was identified as the definitive source of her upper GI hemorrhage Discussion: Gastric diverticula are rare, typically asymptomatic, but may cause epigastric pain (18–30%), nausea, or refractory GERD-like symptoms. Life-threatening complications (bleeding, perforation, diverticulitis, malignancy) are exceedingly rare. Food retention and digestive juices may trigger inflammation, ulceration, or hemorrhage. GD should be considered in obscure upper GI bleeding after excluding common causes. Endoscopy is diagnostic and therapeutic, while CT may detect incidental cases. Surgery (laparoscopic/open) is reserved for recurrent bleeding or perforation. This case highlights GD as a rare but critical bleeding source, emphasizing early endoscopy for diagnosis and management.
Figure: Bleeding Gastric Fundus Diverticulum
Figure: Gastric Fundus Diverticulum with clips
Disclosures: Angelin Raju indicated no relevant financial relationships. Anish Jomy indicated no relevant financial relationships. Gaurav Arora: Eli Lilly – Advisory Committee/Board Member. James Nackley indicated no relevant financial relationships. Anunaya Aashish indicated no relevant financial relationships. Ashni Dudhia indicated no relevant financial relationships. Daniel Gonzalez indicated no relevant financial relationships. Maher Taha indicated no relevant financial relationships. Amna Naveed Butt indicated no relevant financial relationships.
Angelin Raju, MD1, Anish Jomy, MBBS2, Gaurav Arora, MD3, James Nackley, MD1, Anunaya Aashish, MD1, Ashni Dudhia, DO1, Daniel Gonzalez, MD1, Maher Taha, MD4, Amna Naveed Butt, MD5. P6359 - A Hidden Culprit: Gastric Diverticulum Presenting With Life-Threatening Upper GI Bleeding, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Angelin Raju, MD (she/her/hers) photo")