University of Connecticut Health Center Farmington, CT
Hira Khan, MD1, Anjali Rajagopal, MBBS1, Murali Dharan, 2 1University of Connecticut Health Center, Farmington, CT; 2Employed, Farmington, CT Introduction: Emphysematous gastritis (EG) is a rare & lethal entity characterized by infiltration of gas forming microbes within the gastric mucosa.
Case Description/
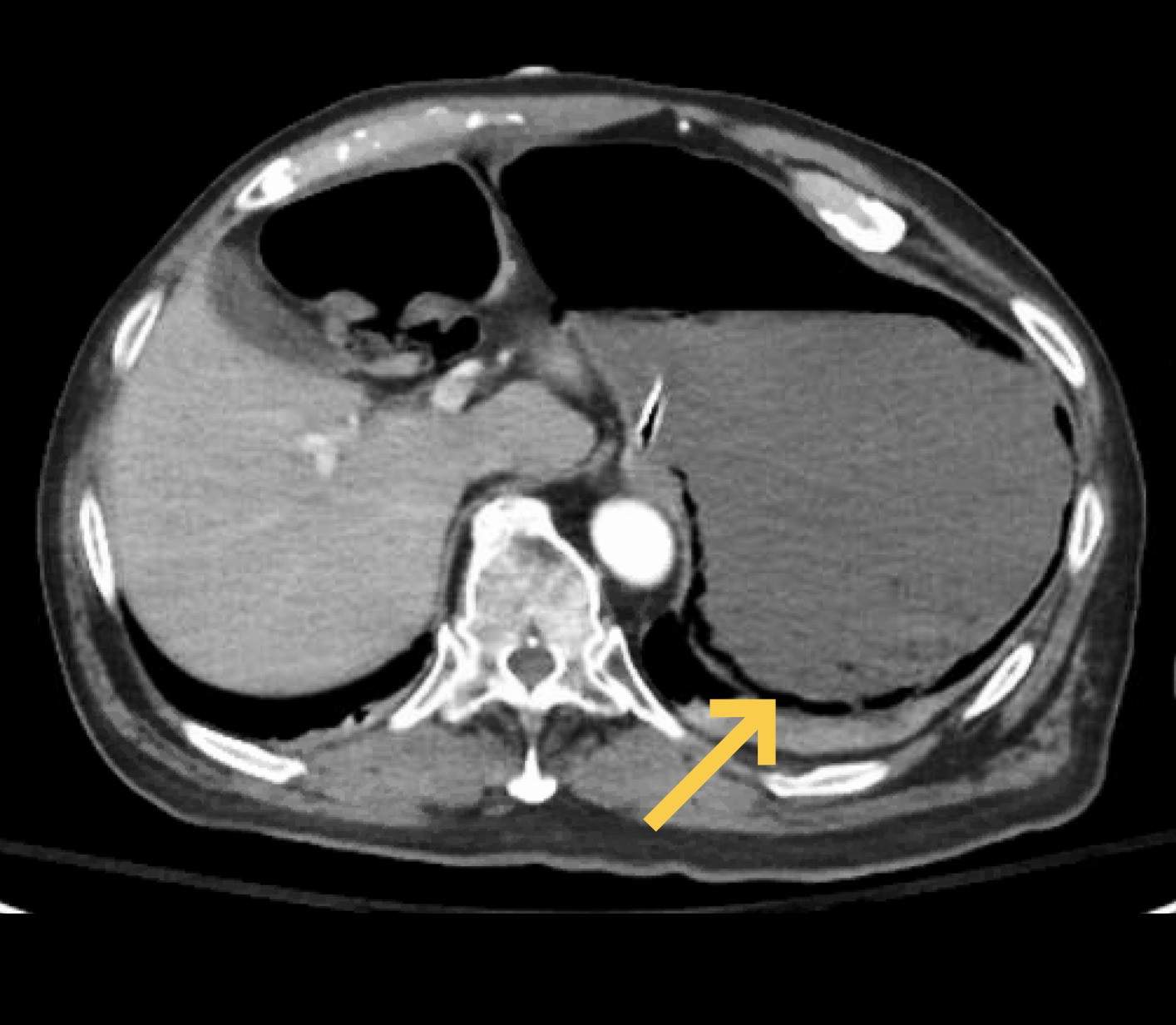
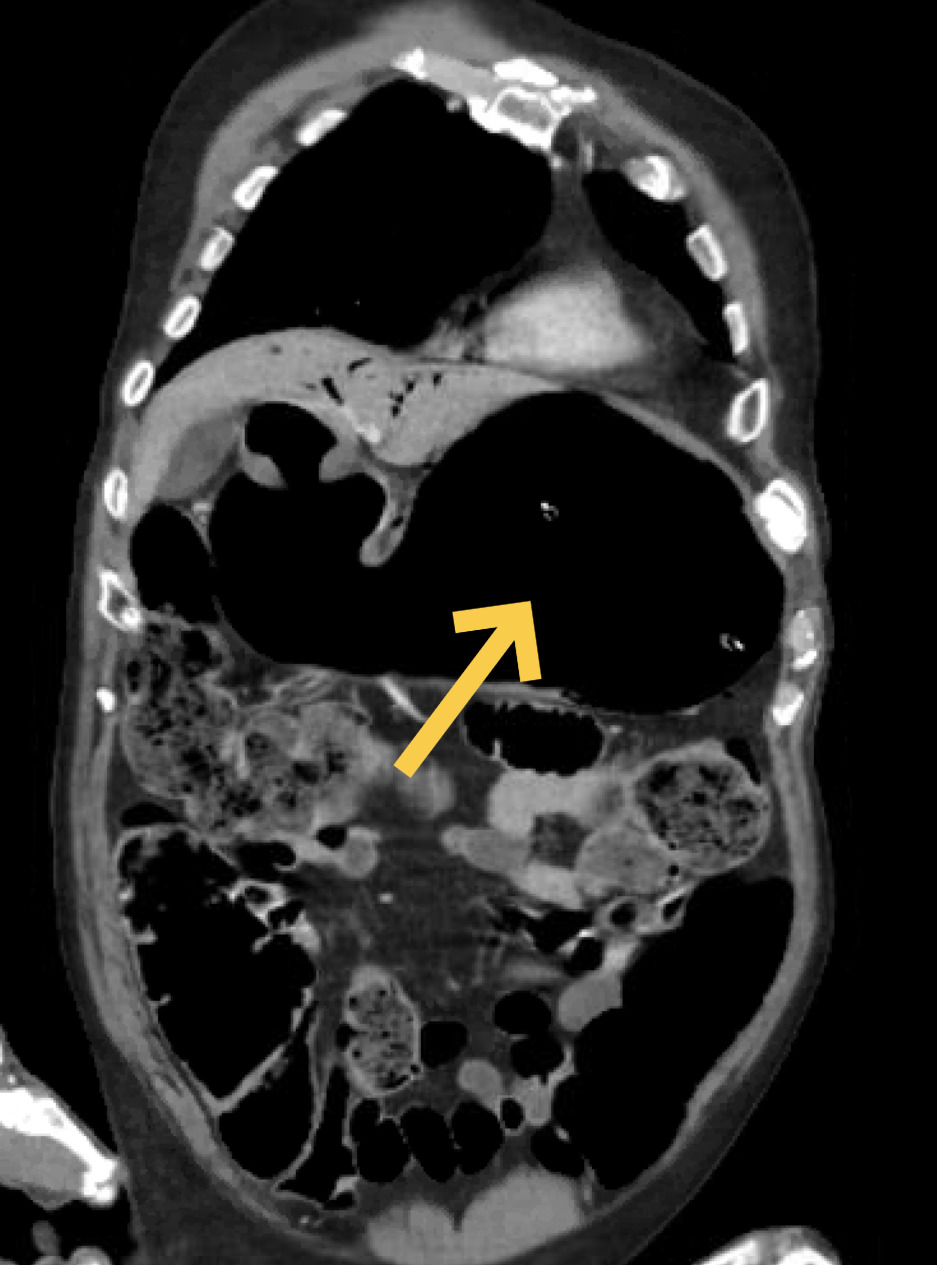
Methods: A 75-year-old male with a past medical history of dementia, hypertension, CKD, & COPD presented in the setting of unresponsiveness, and was admitted for suspected aspiration pneumonia. Vitals were notable for tachycardia & hypotension (95/66 mm Hg). Abdominal tenderness, distension & rigidity were noted on physical exam. Labs revealed an elevated WBC count (13.3 x 10^3/μL), BUN (31 mg/dL), creatinine (1.4 mg/dL) & lactate (3.3 mmol/L). CT A/P revealed a markedly distended stomach & portal venous gas without pneumoperitoneum (Figures 1.0 and 2.0). The esophagus was dilated with severe ostial stenosis of the celiac trunk. Empiric broad spectrum antibiotics & IV PPIs were initiated. Patient was upgraded to the ICU for further management. NG tube placement yielded coffee-ground aspirate. EGD & surgical intervention were deferred due to unfavorable risk benefit profile. Discussion: EG is a life-threatening condition with mortality rates as high as 61%. Patients often present with fulminant shock. Risk factors include gastroenteritis, alcohol use disorder, T2DM, ESRD, prolonged NSAID use, malignancy, caustic ingestion & immunodeficiency. There have been cases linked to severe atherosclerosis with consequent gastrointestinal necrotic lesions which may serve as a nidus for bacterial growth. Definitive diagnosis is through abdominal CT and aspirate culture. Our case demonstrated distension of the stomach with mural gas within the cardia & antrum with presence of left hepatic venous gas. Our patient had severe flow limiting stenosis celiac trunk which serves as the primary arterial supply of the stomach. Our patient also had a concomitant COVID infection. Literature on association between COVID-19 infection & EG is scarce, though there is a postulated risk of invasion of gastrointestinal angiotensin converting enzyme 2 (ACE2) receiver which can promote inflammation, disrupt barrier integrity & promote dysbiosis. Furthermore, hypercoagulability due to the vascular endothelial injury caused by COVID-19 infection may also contribute. Conservative management is with fluid resuscitation & broad-spectrum antibiotics & rarely anti-fungal coverage. Mortality is high, even with definitive surgical management. Our patient continued to deteriorate clinically despite these measures & he ultimately passed.
Figure: Fig 1.0 Axial CT with contrast demonstrating emphysematous gastritis with gastric mural gas
Figure: Fig 2.0 Coronal CT scan showing portal venous gas and marked gastric distention
Disclosures: Hira Khan indicated no relevant financial relationships. Anjali Rajagopal indicated no relevant financial relationships. Murali Dharan indicated no relevant financial relationships.
Hira Khan, MD1, Anjali Rajagopal, MBBS1, Murali Dharan, 2. P6353 - Emphysematous Gastritis in a Patient With COVID Infection and Celiac Artery Stenosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")