Prince Shah-Riar, MD1, Rishika Trivedi, MD2, Mahmoud Barbarawi, MD2, Asif Zamir, MD, FACG3 1DHR Health, Edinburg, Tx, McAllen, TX; 2DHR Health, McAllen, TX; 3DHR Health Gastroenterology, Edinburg, TX Introduction: Smooth, scarred antral stenosis—described endoscopically as "pseudopylorus"—can mislead clinicians into underestimating the malignant potential of gastric outlet obstruction (GOO). When biopsies are obtained from adjacent mucosa and not the pyloric ring itself, underlying carcinoma may remain undetected. This case illustrates how anatomic mis-targeting during repeated endoscopy delayed diagnosis of pyloric adenocarcinoma.
Case Description/
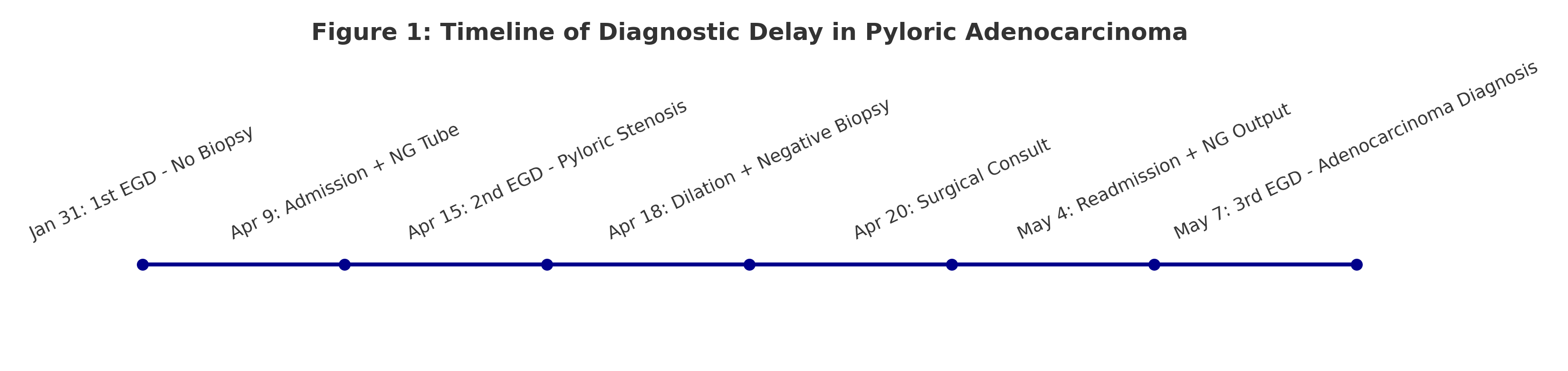
Methods: A 52-year-old man with schizophrenia and type 2 diabetes presented with persistent vomiting, early satiety, and NG output >900 cc/day. Initial EGD (01/31/2025) revealed esophagitis and gastritis; no obstructing lesion was seen. He was managed as presumed diabetic gastroparesis. By April, symptom persistence prompted two further EGDs (04/15 and 04/18), each noting a narrowed but smooth pylorus without ulceration. Biopsies were obtained from the antrum and described as chronic gastritis with reactive changes—no dysplasia or malignancy.
Despite 36 Fr balloon dilation on 04/18, symptoms progressed. A final EGD (05/07/2025) revealed friability and mucosal distortion at the true pyloric ring. Targeted biopsy at that site confirmed moderately differentiated intestinal-type adenocarcinoma, CDX2+, villin+, HER2–. Diagnosis had been delayed >90 days despite multiple endoscopies. Discussion: This case underscores a critical procedural oversight: sampling the antrum adjacent to a narrowing is not equivalent to sampling the stricture itself. The false reassurance of "non-ulcerated narrowing" combined with repeated off-target biopsies led to prolonged diagnostic delay. “Pseudopylorus” should not deter directed pyloric sampling or staging EUS when obstruction is persistent and unexplained. Early histologic confirmation would have altered nutritional, oncologic, and surgical planning. Benign-appearing antral narrowing can harbor malignancy when true pyloric mucosa is bypassed during biopsy. In the setting of refractory GOO, direct sampling of the stenotic channel is essential—even when mucosa appears smooth. This case advocates for endoscopic precision and diagnostic escalation in anatomically deceptive GOO presentations.
Figure: Figure 1: Dated timeline of diagnostic and endoscopic interventions.
Disclosures: Prince Shah-Riar indicated no relevant financial relationships. Rishika Trivedi indicated no relevant financial relationships. Mahmoud Barbarawi indicated no relevant financial relationships. Asif Zamir indicated no relevant financial relationships.
Prince Shah-Riar, MD1, Rishika Trivedi, MD2, Mahmoud Barbarawi, MD2, Asif Zamir, MD, FACG3. P6352 - When Pseudo Pylorus Deceives: Delayed Diagnosis of Pyloric Adenocarcinoma from Missed Targeted Biopsy in Refractory Gastric Outlet Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")