Indiana University School of Medicine Indianapolis, IN
Samreen Jawaid, MD1, Tarek G.. Aridi, MD1, Pedro Escobedo, MD1, Namra Pasha, MBBS2, Marta Arjonilla, MD1, Archita P.. Desai, MD1 1Indiana University School of Medicine, Indianapolis, IN; 2Karachi Medical and Dental College, Karachi, Sindh, Pakistan Introduction: Laparoscopic cholecystectomy is the standard approach for treating acute cholecystitis due to improved patient outcomes, shorter hospital stays, and reduced re-hospitalizations. However, it carries a higher risk of iatrogenic biliary injuries (0.3–0.6%) compared to open cholecystectomy (0.1%). Such injuries can result in rare complications like biloma formation. We present a rare case of an infected post-cholecystectomy biloma within the gallbladder fossa, complicated by secondary sclerosing cholangitis.
Case Description/
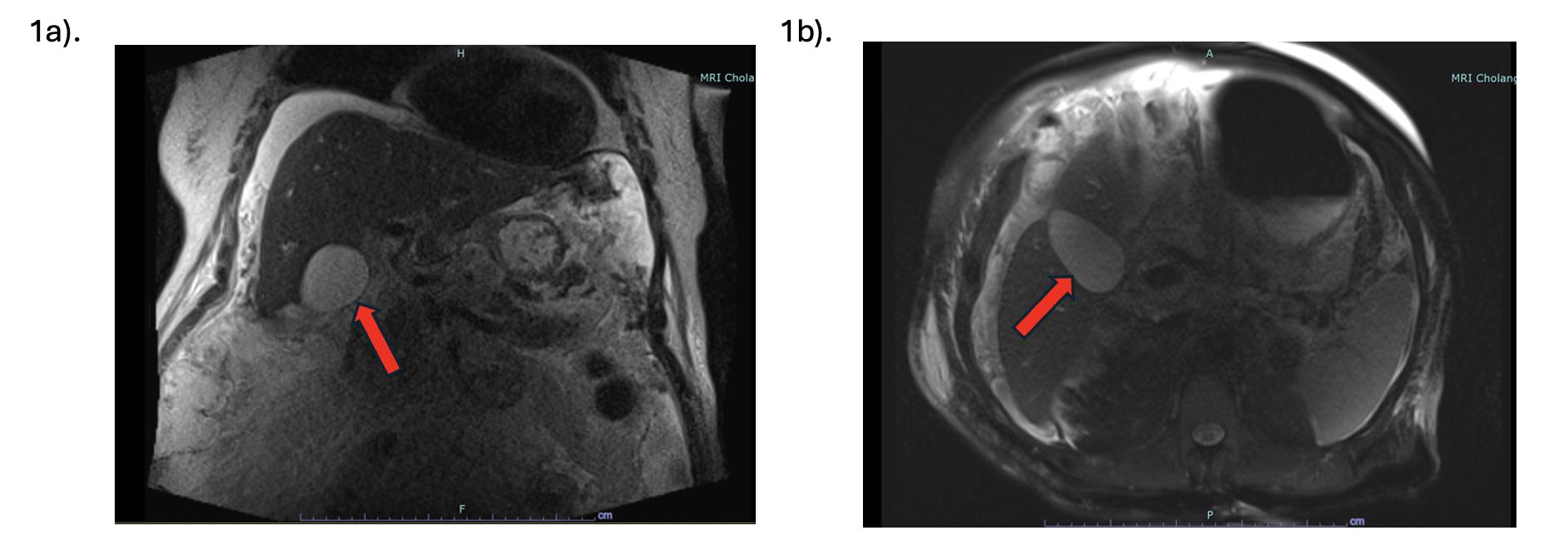
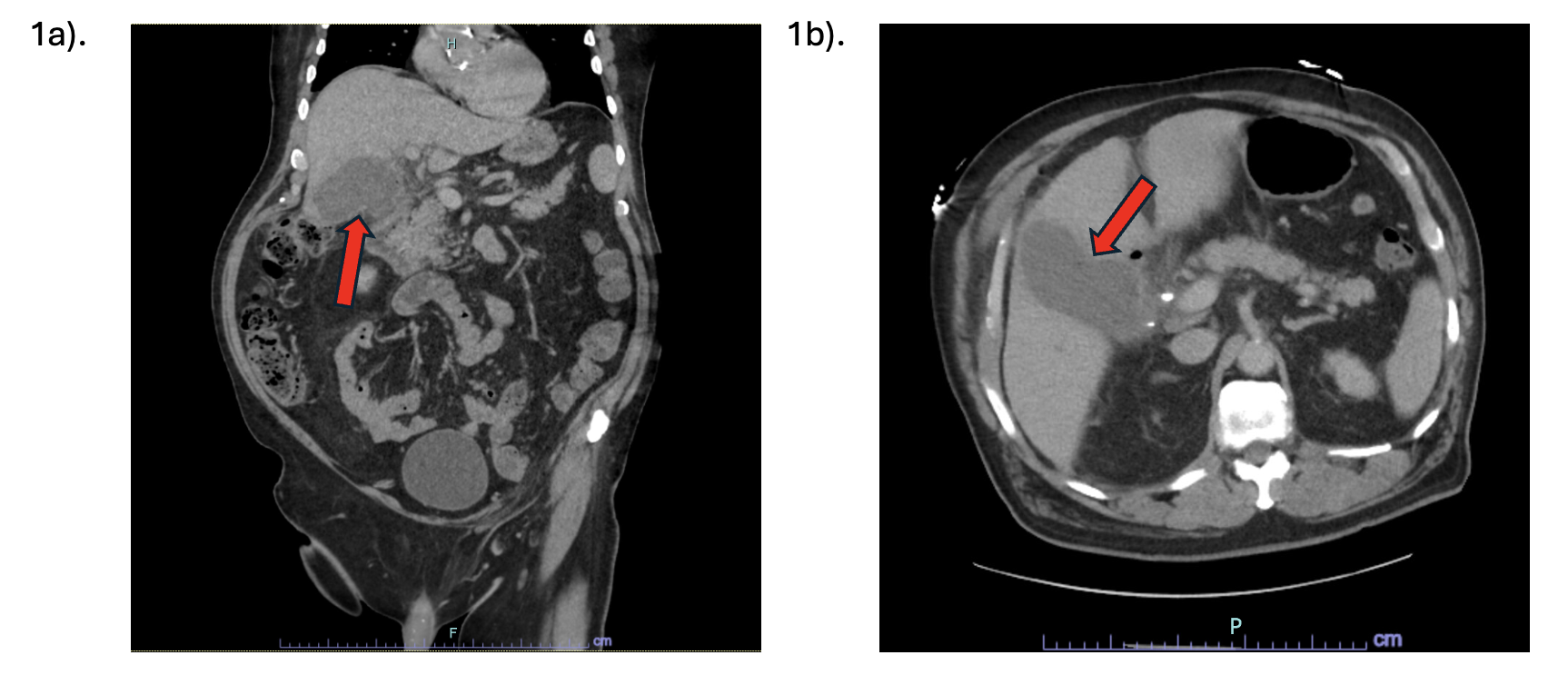
Methods: 69-year-old male with complex medical history, including emphysematous cholecystitis status post laparoscopic cholecystectomy complicated by cholangitis requiring stents, drainage and antibiotics, presented with fatigue, hypotension, and abdominal tenderness. CT abdomen and magnetic resonance cholangiopancreatography (MRCP) revealed a loculated collection with well-defined thin margins in the gallbladder fossa. (Figure 1 and Figure 2). Endoscopic retrograde cholangiopancreatography (ERCP) ruled out a biliary leak but revealed new, diffuse biliary tract stenosis consistent with secondary sclerosing cholangitis. Aspiration of 60 mL of bilious fluid from the fossa grew vancomycin resistant (VRE) Enterococcus faecium and extended spectrum beta lactamase (ESBL) Klebsiella; He was started on meropenem and linezolid. However, the bilious fluid re-accumulated within 48 hours despite no identifiable leak. Subsequently, an intra-hepatic drain was placed. Unfortunately, his course was complicated by acute stress cardiomyopathy, ultimately leading to demise. Discussion: This case reflects on numerous pertinent factors. First, early diagnostic imaging is essential in differentiating bilomas from other fluid collections, such as seromas and abscesses, given the higher risk of mortality especially when infected. However, radiographic appearance is insufficient and direct fluid sampling aids in confirming diagnosis. Second, while ERCP and radionuclide imaging occasionally identify the site of leaks, in many cases, as in ours, the source remains elusive. Therefore, clinical judgment should prioritize timely intervention over definitive localization. Third, infected bilomas require aggressive multidisciplinary management with percutaneous drainage and targeted antibiotics to prevent complications like peritonitis or bilhemia. In summary, infected bilomas, though uncommon, require vigilant monitoring and decisive action to ensure favorable patient outcomes.
Figure: Figure1: CT abdomen/pelvis with loculated collection with clear thin margins in the gallbladder fossa a) Coronal view. b) Axial view.
Figure: Figure 2: MRCP demonstrating a gallbladder fossa collection with well-defined, thin margins a) Coronal view. b) Axial view.
Disclosures: Samreen Jawaid indicated no relevant financial relationships. Tarek Aridi indicated no relevant financial relationships. Pedro Escobedo indicated no relevant financial relationships. Namra Pasha indicated no relevant financial relationships. Marta Arjonilla indicated no relevant financial relationships. Archita Desai: Eli Lilly – Consultant.
Samreen Jawaid, MD1, Tarek G.. Aridi, MD1, Pedro Escobedo, MD1, Namra Pasha, MBBS2, Marta Arjonilla, MD1, Archita P.. Desai, MD1. P2289 - Infected Biloma in the Gallbladder Fossa: A Rare Post-Cholecystectomy Complication, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.