University of South Florida Morsani College of Medicine Tampa, FL
Andres Cordoba, DO1, Francisco Pascual, MD1, Shreya Narayanan, MD2 1University of South Florida Morsani College of Medicine, Tampa, FL; 2University of South Florida Morsani College of Medicine and James A. Haley VA Hospital, Tampa, FL Introduction: Hypertensive emergency is a life-threatening condition defined by severe hypertension and evidence of end-organ damage. Early recognition and initiation of timely management are necessary to reduce significant morbidity and mortality often associated with its presentation. Here, we discuss a unique case of hypertensive emergency due to acute-on-chronic constipation.
Case Description/
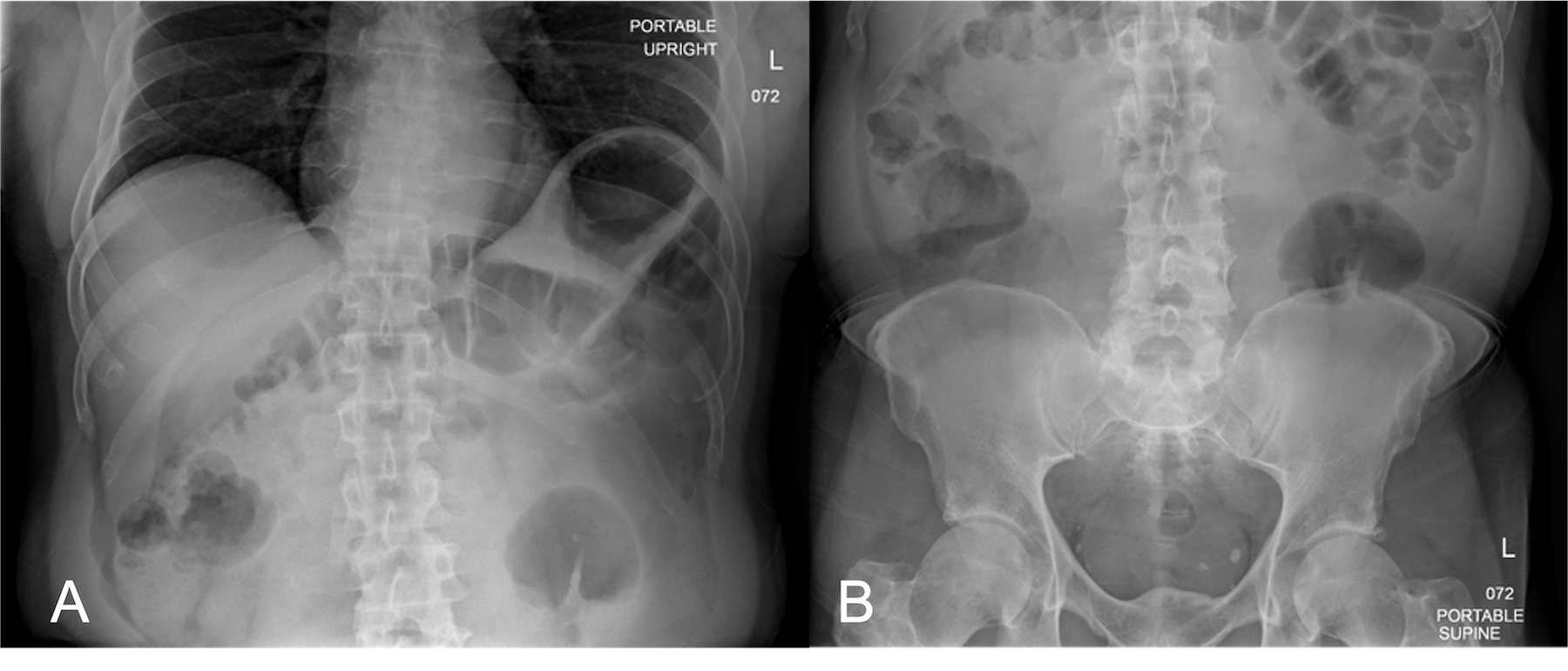
Methods: A 69-year-old male with hyperlipidemia and diabetes presented with four days of diffuse, progressive abdominal pain, nausea, and vomiting. On initial evaluation, his vital signs were notable for new-onset blood pressure elevation to 185/111 mmHg. Despite treatment with oral antihypertensive therapy and intravenous morphine, his symptoms persisted with worsening systolic pressures greater than 200 mmHg. The remainder of his examination was within normal limits, aside from notable tenderness to palpation over his lower abdomen. Laboratory testing revealed elevated high-sensitivity troponin (147 ng/L) and lactic acid (2.7 mmol/L), but blood counts, chemistries, renal and hepatic function, and index EKG were normal. Abdominal X-ray revealed a large stool burden throughout the colon and rectum with gaseous distention of the transverse colon, concerning for fecal impaction. CT angiography of the abdomen revealed neither acute vascular pathology nor evidence of bowel ischemia, but was notable for a large stool burden in the distal ascending colon without evidence of obstruction. He was subsequently started on continuous IV nicardipine and admitted to the cardiac intensive care unit for hypertensive emergency. For his severe constipation, polyethylene glycol, senna, lactulose, and bisacodyl suppositories were administered. Following a large volume bowel movement, he had complete resolution of his abdominal pain and blood pressure normalization. Serial troponins peaked at 185 ng/L and EKGs in parallel were without ischemic change. He was successfully discharged home on hospital day three with a daily bowel regimen and without the need for antihypertensive medications. Discussion: Constipation is a common cause of abdominal discomfort, and severe constipation can precipitate or exacerbate existing hypertension through mechanisms such as increased sympathetic activation due to pain. In cases such as this, it is important to consider this mechanism to provide timely management and attempt to reduce the morbidity and mortality associated with hypertensive emergencies.
Figure: Figure 1. A. Portable Upright Abdominal X-ray B. Portable Supine Abdominal X-ray
Disclosures: Andres Cordoba indicated no relevant financial relationships. Francisco Pascual indicated no relevant financial relationships. Shreya Narayanan indicated no relevant financial relationships.
Andres Cordoba, DO1, Francisco Pascual, MD1, Shreya Narayanan, MD2. P2577 - Hypertensive Emergency: Moving Fast to Correct Slow Transit Constipation, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.