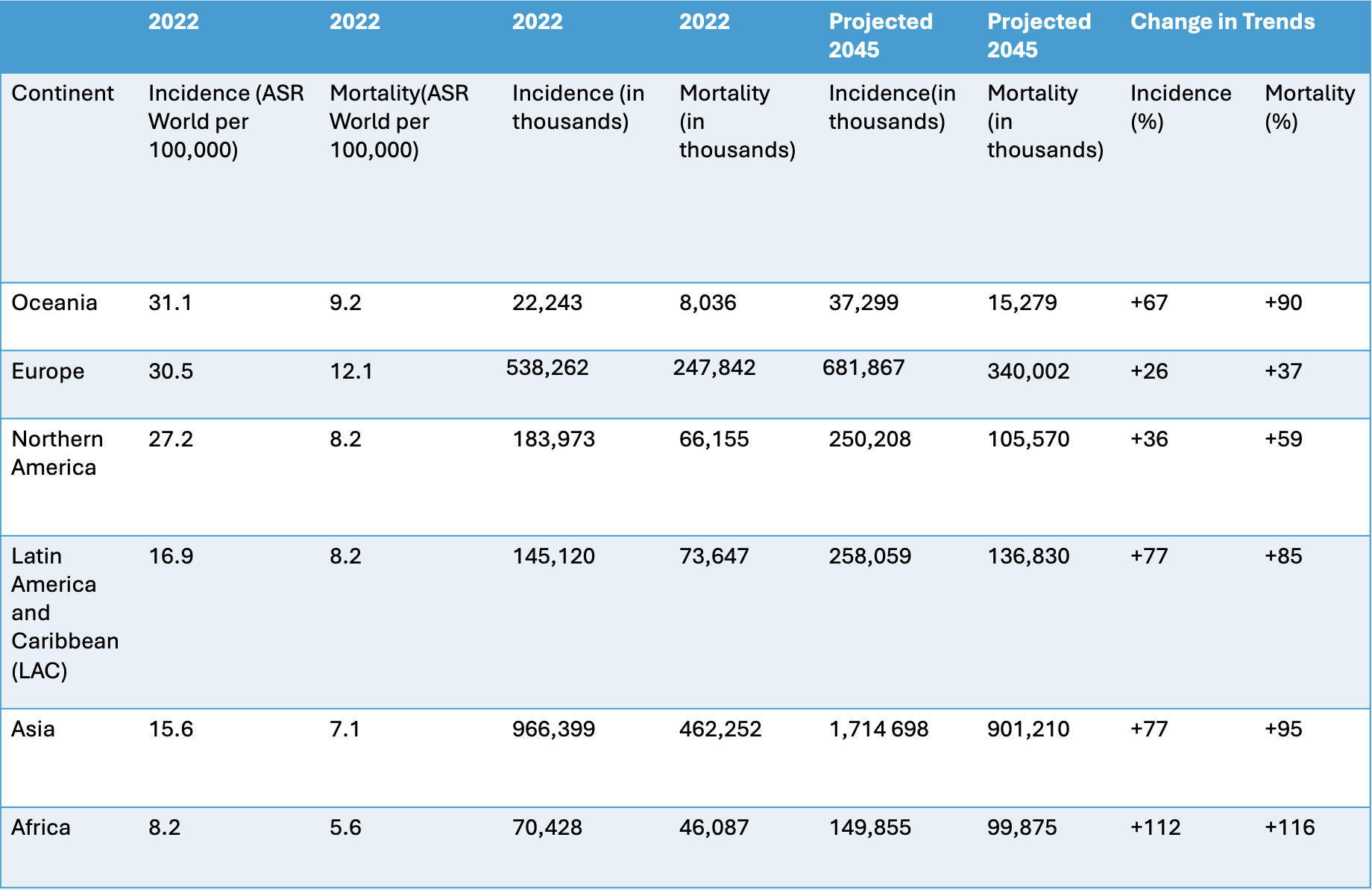
Marquise Soto, MD1, Preethi Jagannath, MBBS2, Simran Joshi, MD3, Jeevin Singh Sandhu, DO4, Matthew Antony. Manoj, MBBS5, Charitha Karanam Ramapathy, MD6, Corinne Caissie, MD3, Pujitha Vallivedu Chennakesavulu, MD, MBBS7, Akshay Sharma, MBBS8, Sushrut Ingawale, MD, DNB, MBBS9 1Massachusetts General Hospital, Chelsea, MA; 2Mount Auburn Hospital, Cambridge, MA; 3Yale New Haven Health, Bridgeport Hospital, Bridgeport, CT; 4Methodist Dallas Medical Center, Dallas, TX; 5Beth Israel Deaconess Medical Center, Boston, MA; 6UAB Montgomery, Montgomery, AL; 7Quinnipiac University Frank H Netter School of Medicine/ St Vincent medical center, Bridgeport, CT; 8Luminis Health Anne Arundel Medical Center, Annapolis, MD; 9Quinnipiac University - Frank H Netter MD School of Medicine, Bridgeport, CT Introduction: Colorectal cancer (CRC) is the third most common cancer and the second leading cause of cancer-related deaths globally. CRC is commonly seen in developed countries and CRC burden is often considered a measure of a country’s development due to the observed trend of increased incidence rates with high or increasing human development index (HDI). Developing nations undergoing rapid growth are seeing increased CRC cases. This review compares CRC incidence and mortality across countries of varying income levels and HDI, highlighting the impact of screening programs on these statistics. Methods: PubMed and EMBASE were systematically searched to identify studies that examined CRC incidence, mortality, and screening programs globally. Over 800 papers were identified, 35 full papers reviewed, and 18 studies were included. Results: Oceania, Europe, and Northern America had the highest age-standardized incidence rates and most cases were from very high HDI and high-income countries (HICs) except for Russia, an upper-middle-income country (UMIC).Europe and Oceania had the highest age-standardized mortality rates. LAC and Asia had the next highest age-standardized incidence rates and most cases were from high HDI nations and UMICs, except for Argentina and Japan, very high HDI countries. Africa had the lowest age-standardized incidence with contributions from high and low HDI nations. Asia and Africa had the lowest age-standardized mortality rates. Reductions in mortality have been reported of 15% in the UK, 18% in Denmark, 30% in Japan, 31.7% in China, and 32% in the U.S. due to annual fecal occult blood screenings. Challenges to implementation of screening in low-income countries (LICs) are lack of a cancer registry, lack of awareness of CRC, poor health system infrastructure, and inadequate financial resources. Discussion: The major burden of CRC is seen in high HDI countries and UMIC to HICs. There is a need for improved screening uptake in HICs and UMICs to reduce the global CRC burden. Mortality rates are impacted by the quality of the screening methods and population-based screening of average-risk individuals is the most effective method for nations with resources. For resource-limited countries, opportunistic screening of high-risk patients may be effective. Cancer registries and educational programs would also benefit LICs. Further studies, should focus on comparing screening uptake in countries with higher mortality rates and validating screening modalities for resource-limited countries.
Figure: Table 1 Global cancer observatory (GLOBOCAN) data on incidence and mortality rates by continent
Disclosures: Marquise Soto indicated no relevant financial relationships. Preethi Jagannath indicated no relevant financial relationships. Simran Joshi indicated no relevant financial relationships. Jeevin Singh Sandhu indicated no relevant financial relationships. Matthew Manoj indicated no relevant financial relationships. Charitha Karanam Ramapathy indicated no relevant financial relationships. Corinne Caissie indicated no relevant financial relationships. Pujitha Vallivedu Chennakesavulu indicated no relevant financial relationships. Akshay Sharma indicated no relevant financial relationships. Sushrut Ingawale indicated no relevant financial relationships.
Marquise Soto, MD1, Preethi Jagannath, MBBS2, Simran Joshi, MD3, Jeevin Singh Sandhu, DO4, Matthew Antony. Manoj, MBBS5, Charitha Karanam Ramapathy, MD6, Corinne Caissie, MD3, Pujitha Vallivedu Chennakesavulu, MD, MBBS7, Akshay Sharma, MBBS8, Sushrut Ingawale, MD, DNB, MBBS9. P2661 - A Systematic Review of Colorectal Cancer Incidence, Mortality, and Screening in Low, Middle, and High Income Countries, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")