Orlando VA Medical Center and UCF/HCA Greater Orlando Kissimmee, FL
Syed Usman Mumtaz, DO1, Saud Khan, MD1, Sohaib Ahmed, DO1, Nabiha Atiquzzaman, BS2, Seth Lipka, MD3 1Orlando VA Medical Center and UCF/HCA Greater Orlando, Kissimmee, FL; 2Nova Southeastern University, Kissimmee, FL; 3Digestive and Liver Center of Florida, Orlando, FL Introduction: Lymphocytic esophagitis (LE) is characterized by infiltration of lymphocytes within the epithelium. This rare (0.1%) ¹, condition typically affects middle-aged individuals with female predominance, ² commonly presenting with dysphagia and heartburn, chest pain, or food impaction. Endoscopic findings vary from normal to erosive esophagitis, esophageal rings, furrows, or stenosis. LE is associated with gastroesophageal reflux disease (GERD), primary esophageal motility disorders, IBD, and autoimmune conditions.
Case Description/
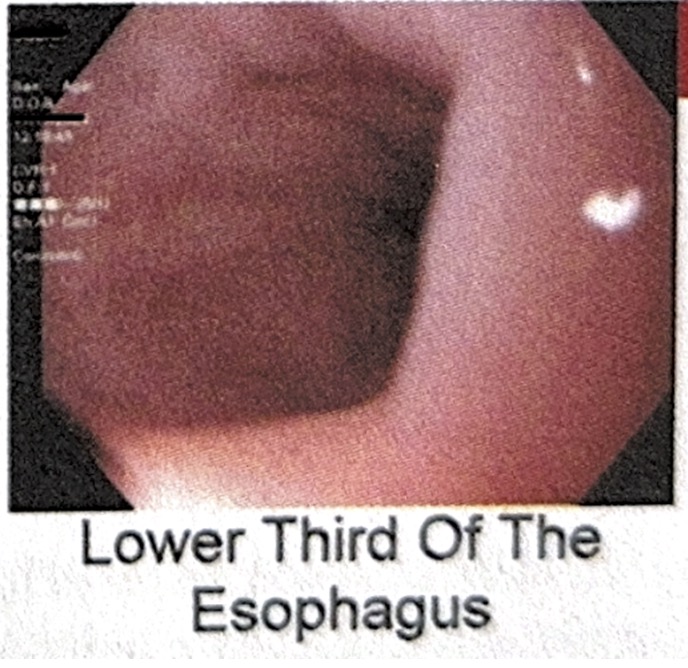
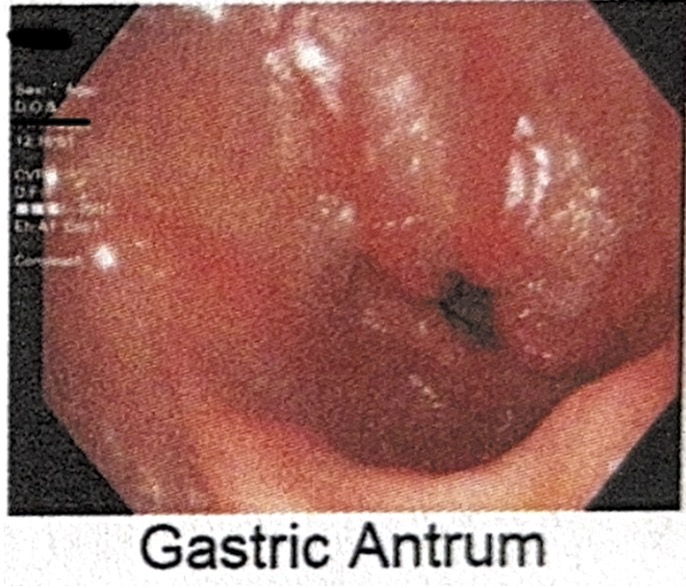
Methods: A 47-year-old male with a history of GERD, type 2 diabetes and active tobacco use presented with 6 months of intermittent dysphagia, globus sensation, nausea and treatment resistant heartburn. Initial evaluation was unrevealing. The patient underwent endoscopy (figures 1,2), revealing normal appearing esophagus and duodenum, and diffuse moderate inflammation throughout the stomach. Biopsies revealed chronic inflammation in the stomach and increased intraepithelial lymphocytes with spongiosis and minimal granulocytic infiltration of the esophagus. No evidence of eosinophilic esophagitis, celiac disease, or H. Pylori was identified. The patient was given a 30-day course of oral budesonide solution with significant improvement in symptoms but was lost to follow-up due to relocation. Discussion: LE classically presents with globus sensation, heartburn, and most commonly dysphagia.¹ Nocturnal heartburn and tobacco use are potential risk factors.² The coexistence of chronic gastritis suggests an underlying systemic inflammatory etiology.³ The pathophysiology of LE remains incompletely understood, though theories propose LE represents a nonspecific immune mediated inflammatory pattern triggered by conditions such as GERD, motility disorders, and systemic immune pathology.4,5 The natural history of LE is generally benign, with most patients exhibiting improvement with treatment. Potential complications include esophageal strictures, food impaction, and rarely esophageal perforation. Excellent response to topical budesonide supports recent literature favoring anti-inflammatory treatment. Long term follow-up data remains limited due to the relatively recent recognition of this condition.
Figure: Figure 1: Lower Third of Esophagus
Figure: Figure 2: Gastric Antrum
Disclosures: Syed Usman Mumtaz indicated no relevant financial relationships. Saud Khan indicated no relevant financial relationships. Sohaib Ahmed indicated no relevant financial relationships. Nabiha Atiquzzaman indicated no relevant financial relationships. Seth Lipka indicated no relevant financial relationships.
Syed Usman Mumtaz, DO1, Saud Khan, MD1, Sohaib Ahmed, DO1, Nabiha Atiquzzaman, BS2, Seth Lipka, MD3. P2838 - Rare Case of Lymphocytic Esophagitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")