Wilfor Diaz Fernandez, MD1, Cadman Leggett, MD2 1Mayo Clinic, Boston, MA; 2Mayo Clinic, Rochester, MN Introduction: Early gastroesophageal cancer (GE) commonly presents without distant disease. The development of locoregional lymphadenopathy and acute pulmonary embolism in these cases rises the concern for metastatic disease. We present the case of Coccidioides lymphadenitis complicating the course and management of GE cancer.
Case Description/
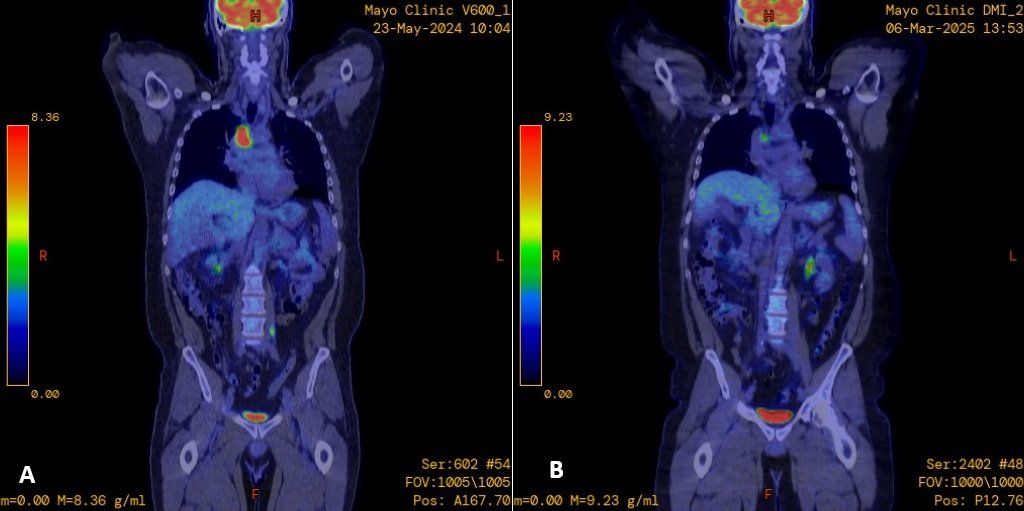
Methods: A 51-year-old Hispanic man was referred to our practice for an incidental diagnosis of a gastroesophageal junction (GEJ) mass detected on esophagogastroduodenoscopy, performed at patient’s request concurrently with a screening colonoscopy. The lesion was removed piecemeal by endoscopic mucosal resection with histopathology demonstrating moderately-to-poorly differentiated intramucosal adenocarcinoma (T1a) with negative deep margins and absence of lymphovascular invasion. Computed tomography (CT) of the chest/abdomen/pelvis showed a subsegmental pulmonary embolism in the posterior right lower lobe as well as an enlarged right lower paratracheal lymph node. A positron emission tomography (PET) scan (Figure 1A) demonstrated multiple mediastinal fluorodeoxyglucose avid lymph nodes, concerning for metastatic disease. The patient subsequently underwent endoscopic bronchial ultrasound with fine needle aspiration (Figure 2) demonstrating granulomatous inflammation with no evidence of malignancy. Bronchoscopy with bronchioalveolar lavage grew saprophytic fungus on fungal culture. Immunodiffusion test results were consistent with an acute Coccidioides infection (positive IgM). The patient was diagnosed with coccidioidal lymphadenitis and treated with a 3 month course of fluconazole 400 mg daily. Subsequent immunodiffusion test and PET scan showed resolution of abnormalities (Figure 1B). Multiple surveillance endoscopies and endoscopic ultrasounds demonstrated complete eradication of his GEJ cancer with no evidence of recurrence. Discussion: Early gastroesophageal cancer (stage T1a) is associated with a low risk of locoregional and metastatic disease (1-2%). Patients with low-risk T1a gastroesophageal adenocarcinomas who present with locoregional lymphadenopathy require further investigation to rule-out alternative etiologies to this finding. Our patient’s mediastinal lymphadenopathy was found to be secondary to Coccidioides lymphadenitis; this condition is caused by Coccidioides immitis or Coccidioides posadasii. Coccidial infections are generally asymptomatic in immunocompetent individuals and isolated lymphatic coccidioides without pulmonary disease is rare.
Figure: Figure 1: A) PET scan showing right paratracheal and precarinal node increased FDG avidity. B) Decrease size and FDG uptake within R paratracheal nodes after course of fluconazole.
Figure: Figure 2:Targeted station 4R EBUS + FNA based on the PET scan
Disclosures: Wilfor Diaz Fernandez indicated no relevant financial relationships. Cadman Leggett indicated no relevant financial relationships.
Wilfor Diaz Fernandez, MD1, Cadman Leggett, MD2. P2832 - From Presumed Metastasis to Chronic Infection: Coccidioidomycosis Mimicking Metastatic Esophageal Adenocarcinoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Wilfor Diaz Fernandez, MD (he/him/his) photo")