Vatsal Khanna, MD1, Bernadette Schmidt, MD2, Jai Kumar, MD3, Julia Greer, MD4 1Henry Ford Health, Southfield, MI; 2Henry Ford Health, Rochester Hills, MI; 3Wayne State University School of Medicine / Ascension Providence Rochester Hospital, Rochester, MI; 4Henry Ford Health, Novi, MI Introduction: Anterior cervical decompression and fusion (ACDF) is an effective procedure for treatment of cervical spondylotic disease. Esophageal fistula after anterior cervical surgeries is rare but potentially fatal, with an incidence of 0.04%–0.25%. We report a case of delayed esophageal perforation presenting as esophageal fistula in an 80-year-old female, occurring 15 years after ACDF.
Case Description/
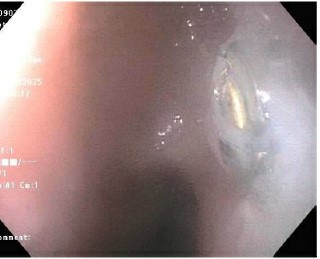
Methods: The patient is an 80-year-old female with a history of cervical stenosis status post C3–C6 ACDF done 15 years ago, who presented to the hospital with complaints of shortness of breath, productive cough associated with food intake, and fever for 1 week. Labs on admission showed a white count of 20,000, hemoglobin 11.0, and basic metabolic panel was within normal limits. Chest X-ray was unremarkable. Computed tomography (CT) of the neck with contrast showed a fistulous tract and air-containing abscess in the deep left neck ventral to the C5, C6, and C7 levels, communicating with a thick-walled and apparently inflamed esophagus. X-ray esophagram was done subsequently, showing a posterior esophageal fistula at the level of C6–C7 with gas and contrast within the prevertebral soft tissues (Figure 1). The patient was started on intravenous ampicillin-sulbactam 3 grams every 6 hours. Gastroenterology was consulted, and the patient underwent esophagogastroduodenoscopy (EGD), which revealed a small fistula in the upper third of the esophagus, 3 cm below the upper esophageal sphincter, and a cervical fixation screw penetrating the esophagus at that level; no fistula closure was attempted (Figure 2). Neurosurgery and otolaryngology services were consulted. The patient underwent removal of anterior cervical spine hardware and esophageal repair with placement of a left sternocleidomastoid flap. Postoperative period was uneventful. A percutaneous gastrostomy tube was placed for enteral nutrition. The patient was advised to remain nil per os and follow up with the surgical teams in the outpatient setting in 2 weeks. Discussion: Esophageal injury related to ACDF is uncommon and may occur after a long postoperative period, affecting prognosis and mortality. A high index of suspicion and early treatment improve outcomes. Management should be individualized based on timing, location, and cause, with supportive measures (e.g., wound care, adequate feeding) as important as surgical repair.
Figure: Figure 1
Figure: Figure 2
Disclosures: Vatsal Khanna indicated no relevant financial relationships. Bernadette Schmidt indicated no relevant financial relationships. Jai Kumar indicated no relevant financial relationships. Julia Greer indicated no relevant financial relationships.
Vatsal Khanna, MD1, Bernadette Schmidt, MD2, Jai Kumar, MD3, Julia Greer, MD4. P2829 - Delayed Esophageal Fistula Following Anterior Cervical Discectomy and Fusion - A Rare Long Term Complication, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Vatsal Khanna, MD photo")