P3066 - Increased Mortality, Hospital Length of Stay, and Health Care Costs for Lower Gastrointestinal Bleeding Among Elderly Adults: Results From a Nationwide Analysis
Renaissance School of Medicine at Stony Brook University Port Jeff Station, NY
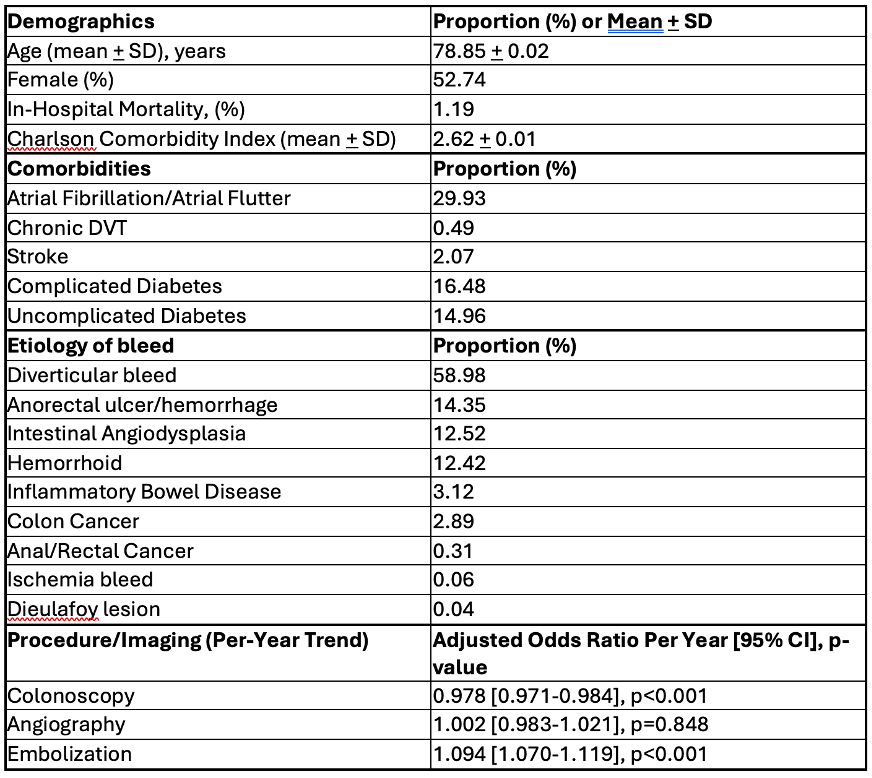
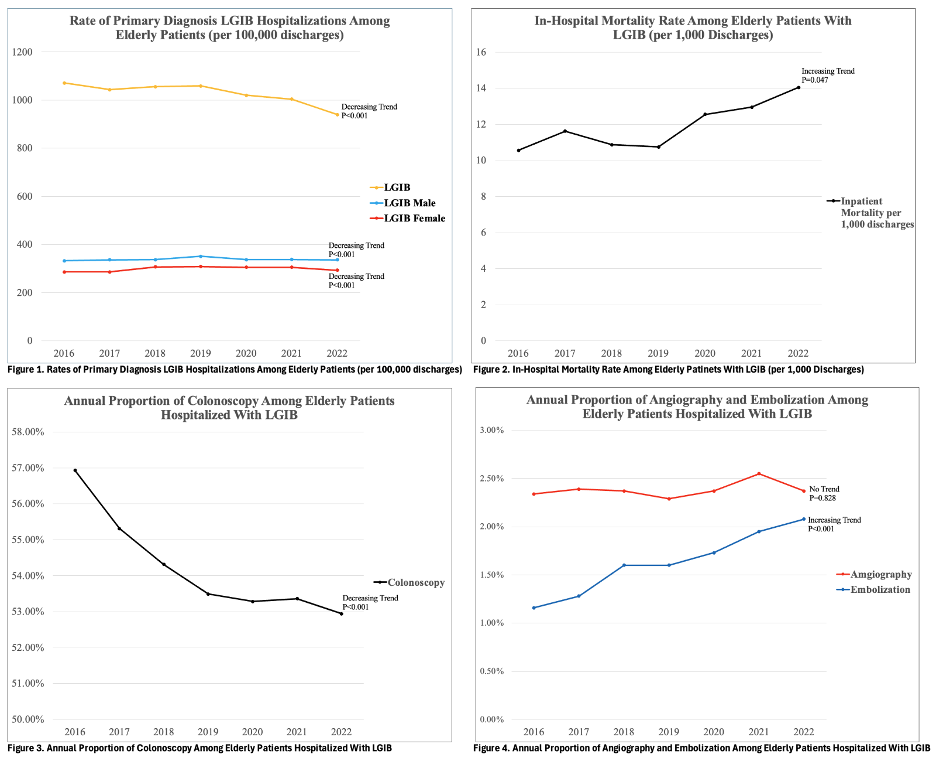
Ballakur Rao, MD1, James Lee, MD2, Jasmine Lee, MD3, Rahul Tripathi, MD2, Daniel Jamorabo, MD4 1Renaissance School of Medicine at Stony Brook University, Stony Brook, NY; 2Stony Brook Medicine, Stony Brook, NY; 3Jefferson Health, Philadelphia, PA; 4Northwell Health, Forest Hills, NY Introduction: Lower gastrointestinal bleeding (LGIB) is a common and significant cause of morbidity in the elderly population. However, national trends in LGIB hospitalizations among older adults remain understudied. Evaluating trends in incidence, mortality, and interventions may offer insight into the evolving burden of LGIB in this population. Methods: We performed a retrospective analysis using the National Inpatient Sample (NIS) from 2016–2022, identifying non-elective hospitalizations for patients aged >65 with LGIB using ICD-10 codes. Outcomes included annual incidence, in-hospital mortality, length of stay (LOS), total hospital charges, and use of colonoscopy, angiography, and embolization. Trend analyses were conducted, and survey weighted logistic and linear regression models were used to evaluate changes over time, adjusting for patient and hospital characteristics. Results: The incidence of LGIB per 100,000 hospital discharges decreased from 1,071 in 2016 to 940 in 2022 (aOR 0.987 [0.983–0.990], p < 0.001). Male patients consistently had a higher incidence compared to females; however, the rate of decline was more pronounced in males (male: aOR 0.981 [0.977–0.986] vs. female: aOR 0.991 [0.987–0.995], p < 0.001). The most common etiologies of LGIB were diverticular bleeding, anorectal hemorrhage/ulcer, angiodysplasia, and hemorrhoids, respectively (Table 1). Over the study period, in-hospital mortality increased from 10.56 per 1,000 discharges in 2016 to 14.04 in 2022 (aOR 1.0257 [1.021–1.071], p = 0.047). Mean hospital charges rose from $40,617.81 in 2016 to $62,133.06 in 2022, with an average annual increase of $3,218 [3,218–3,489], p < 0.001. Average LOS increased from 4.32 to 4.88 days, corresponding to an adjusted annual increase of 0.068 days [0.056–0.081], p < 0.001. There was a small but significant decrease in colonoscopy utilization over time, while embolization use increased, and angiography rates remained unchanged (Table 1). Discussion: While the incidence of LGIB in elderly patients declined over time, the overall burden has increased due to rising mortality, prolonged hospitalizations, and escalating healthcare costs. The modest decrease in colonoscopy use alongside increased embolization may reflect evolving management strategies. These patterns may have been influenced by the COVID-19 pandemic, which disrupted routine care, particularly during 2020–2022. Continued efforts are needed to optimize care delivery and resource utilization for LGIB in the aging population.
Figure: Table 1: Baseline Characteristics
Figure: Image 1: Trends in Hospitalization, In-Hospital Mortality, and Interventions in Elderly Patients Hospitalized with LGIB from 2016 - 2022
Disclosures: Ballakur Rao indicated no relevant financial relationships. James Lee indicated no relevant financial relationships. Jasmine Lee indicated no relevant financial relationships. Rahul Tripathi indicated no relevant financial relationships. Daniel Jamorabo indicated no relevant financial relationships.
Ballakur Rao, MD1, James Lee, MD2, Jasmine Lee, MD3, Rahul Tripathi, MD2, Daniel Jamorabo, MD4. P3066 - Increased Mortality, Hospital Length of Stay, and Health Care Costs for Lower Gastrointestinal Bleeding Among Elderly Adults: Results From a Nationwide Analysis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.