Yale New Haven Health, Bridgeport Hospital Bridgeport, CT
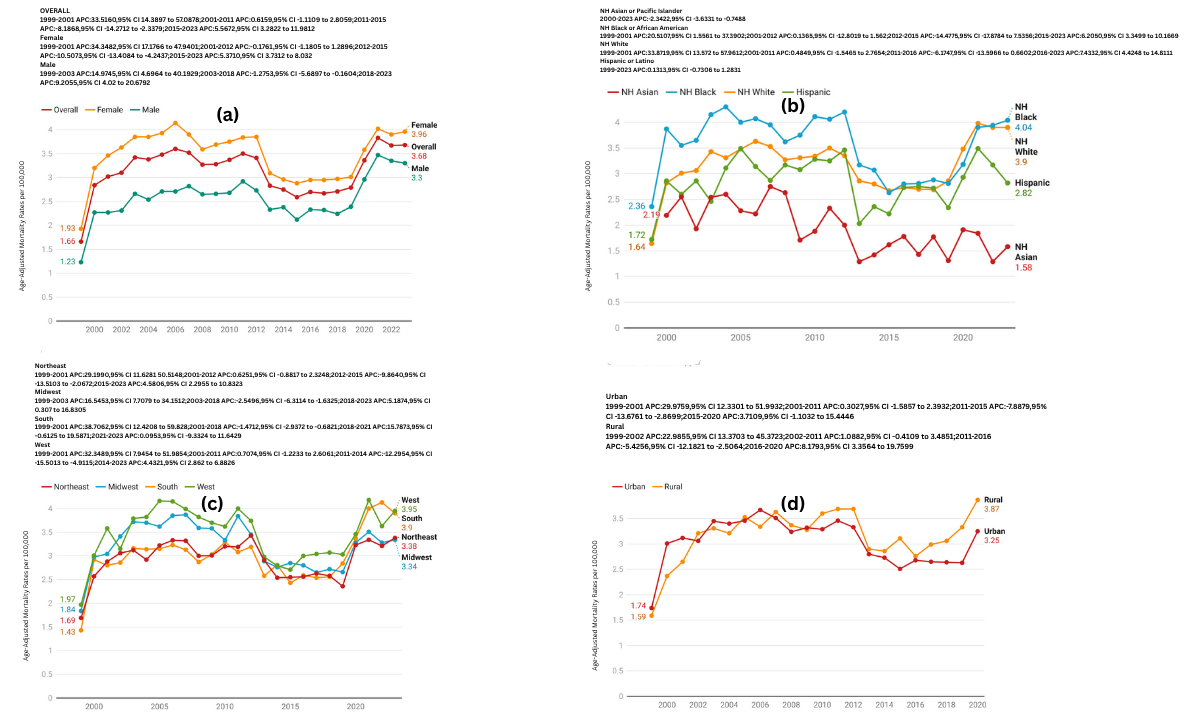
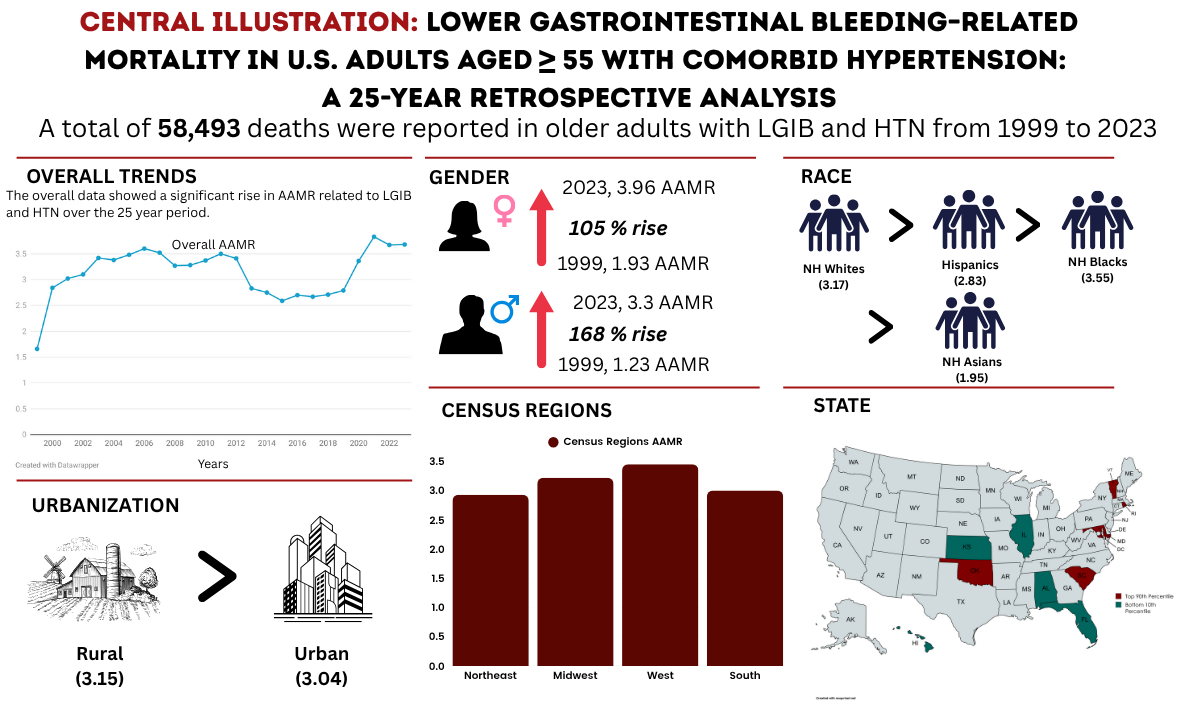
Simran Joshi, MD1, Muhammad Faizan Ali, MD2, Husnain Ahmad, MBBS3, Muhammad Yamman bin irfan, MD4, Corinne Caissie, MD1, Muhammad Hermain Amin, MBBS3, Muhammad Khan, MBBS5, Sherif Eltawansy, MD6, Saman Javaid, MBBS7, Noor ul Ain Saleem, 8, Jeevin Singh Sandhu, DO9, Matthew Antony. Manoj, MBBS10, Marquise Soto, MD11, Mohammad Islam, MD12, Cheng-Hung Tai, MD1 1Yale New Haven Health, Bridgeport Hospital, Bridgeport, CT; 2Jinnah Postgraduate Medical Centre, Karachi, Sindh, Pakistan; 3Shalamar Institute of Health Sciences, Lahore, Punjab, Pakistan; 4Shalamar Institute of Health Sciences, Lahore, Islamabad, Pakistan; 5Bacha Khan Medical College, Mardan, Punjab, Pakistan; 6Jersey Shore University Medical Center, Jersey Shore, NJ; 7CMH Kharian, Sarghoda, Punjab, Pakistan; 8Fatima Memorial Hospital, Lahore, Punjab, Pakistan; 9Methodist Dallas Medical Center, Dallas, TX; 10Beth Israel Deaconess Medical Center, Boston, MA; 11Massachusetts General Hospital, Chelsea, MA; 12Yale New Haven Health, Bridgeport, CT Introduction: Lower gastrointestinal bleeding (LGIB) remains a significant cause of morbidity and mortality among older adults in the United States. Hypertension (HTN), a prevalent comorbidity in this population, may exacerbate bleeding risk through vascular fragility and impaired hemodynamic compensation. Despite growing recognition of the intersection between cardiovascular and gastrointestinal pathology, national data evaluating the burden of LGIB-related mortality among hypertensive individuals remain limited. This study evaluates 25-year trends in LGIB-related mortality among U.S. adults aged ≥55 with comorbid HTN, highlighting disparities across demographic and geographic subgroups. Methods: Mortality data was extracted from the CDC WONDER database (1999–2023) using ICD-10 codes for LGIB and HTN. Age-adjusted mortality rates (AAMRs) per 100,000 were calculated using the 2000 U.S. standard population. Joinpoint regression identified Annual Percent Change (APC) and Average Annual Percent Change (AAPC), with p < 0.05 considered significant. Analyses were stratified by sex, age, race/ethnicity, region, urbanization, and state. Results: There were 58,493 LGIB and HTN-related deaths, with 64.3% occurring in inpatient settings. The AAMR rose 122% from 1.66 (1999) to 3.68 (2023) (AAPC: 3.0%, 95% CI: 2.3–4.4, p < 0.000001). Women had a 36% higher mortality rate than men (3.4 vs. 2.5), though men showed a faster rise (AAPC: 3.4% vs. 2.7%). Adults aged 75+ had much higher AAMRs than those aged 55–74 (8.0 vs. 1.2), but the younger group saw steeper increases (AAPC: 3.9% vs. 2.7%). Non-Hispanic (NH) Blacks had the highest AAMR (3.5), while NH Whites experienced the sharpest rise (AAPC: 3.4%, p < 0.000001). Regionally, the West had the highest AAMR (3.4), and the South had the steepest increase (AAPC: 3.5%). Rural areas had slightly higher AAMRs than urban areas (3.15 vs. 3.04) and a faster rise (AAPC: 3.6% vs. 1.9%). States in the top 90th percentile included Rhode Island, South Carolina, Oklahoma, Vermont, and Maryland. Discussion: LGIB and HTN-related mortality has more than doubled over two decades, with steeper increases in men, NH Whites, adults aged 55–74, individuals residing in rural areas and the South region. These findings highlight the need for integrated care strategies for individuals with LGIB and comorbid hypertension, especially in high-risk populations and underserved regions.
Figure: Trends in lower gastrointestinal bleeding-related mortality in U.S adults aged > 55 with comorbid hypertension
Figure: Central illustration: Lower gastrointestinal bleeding-related morality in U.S adults aged > 55 with comorbid hypertension
Disclosures: Simran Joshi indicated no relevant financial relationships. Muhammad Faizan Ali indicated no relevant financial relationships. Husnain Ahmad indicated no relevant financial relationships. Muhammad Yamman bin irfan indicated no relevant financial relationships. Corinne Caissie indicated no relevant financial relationships. Muhammad Hermain Amin indicated no relevant financial relationships. Muhammad Khan indicated no relevant financial relationships. Sherif Eltawansy indicated no relevant financial relationships. Saman Javaid indicated no relevant financial relationships. Noor ul Ain Saleem indicated no relevant financial relationships. Jeevin Singh Sandhu indicated no relevant financial relationships. Matthew Manoj indicated no relevant financial relationships. Marquise Soto indicated no relevant financial relationships. Mohammad Islam indicated no relevant financial relationships. Cheng-Hung Tai indicated no relevant financial relationships.
Simran Joshi, MD1, Muhammad Faizan Ali, MD2, Husnain Ahmad, MBBS3, Muhammad Yamman bin irfan, MD4, Corinne Caissie, MD1, Muhammad Hermain Amin, MBBS3, Muhammad Khan, MBBS5, Sherif Eltawansy, MD6, Saman Javaid, MBBS7, Noor ul Ain Saleem, 8, Jeevin Singh Sandhu, DO9, Matthew Antony. Manoj, MBBS10, Marquise Soto, MD11, Mohammad Islam, MD12, Cheng-Hung Tai, MD1. P3052 - Lower Gastrointestinal Bleeding–Related Mortality in US Adults Aged ≥ 55 With Comorbid Hypertension: A 25-Year Retrospective Analysis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.