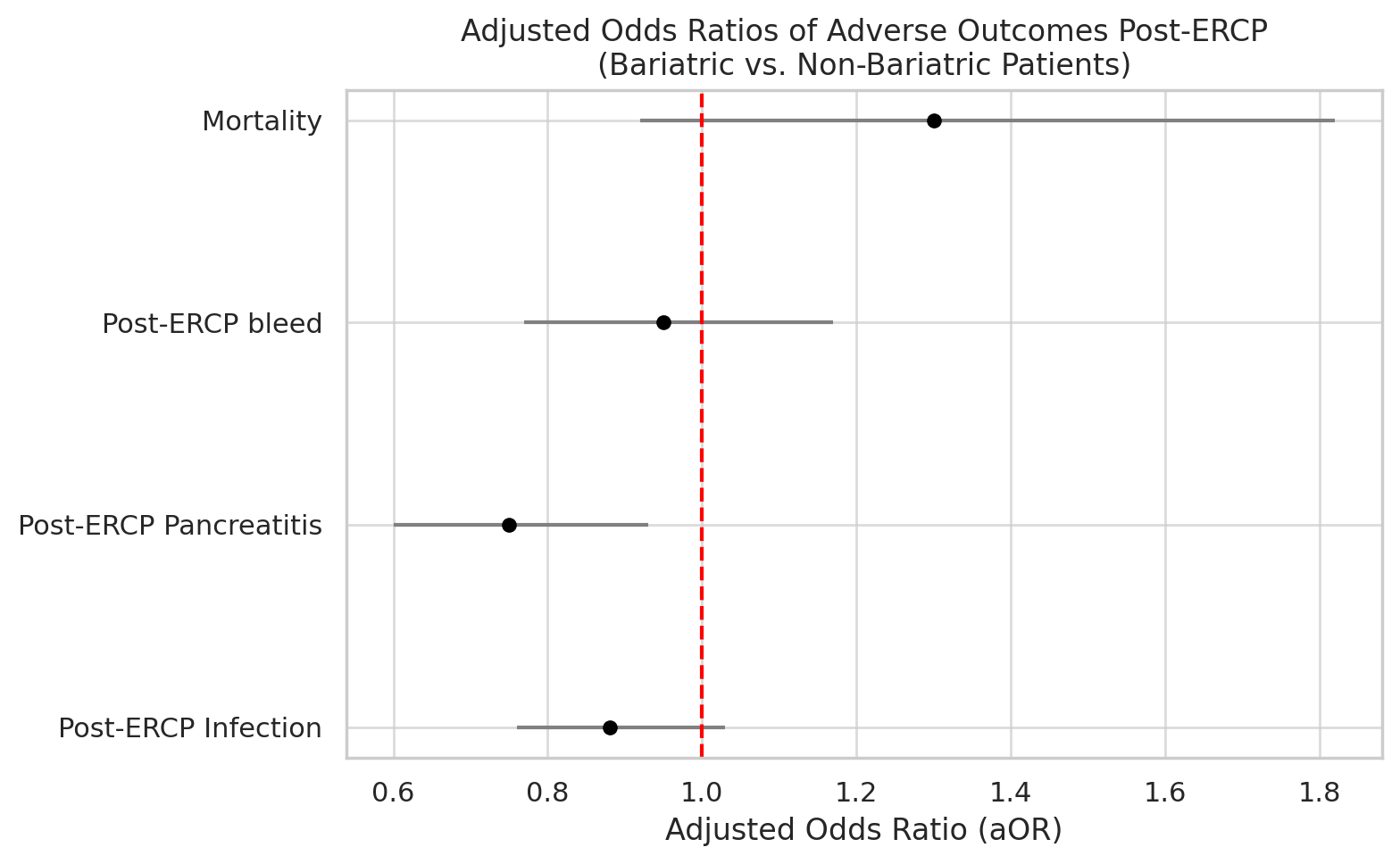
Sarah Meribout, MD1, Ahmed Salem, MD1, Anis Meribout, MD2, Saida Benmostefa, MS3, Ovanes Karslyan, MD1, Urmil Shah, MD4, Kamal Hassan, MD5, Fatima Khan, MD1, Nakul Mahajan, MBBS1, Yasutoshi Shiratori, MD1 1Maimonides Medical Center, Brooklyn, NY; 2Icahn School of Medicine at Mount Sinai, Brooklyn, NY; 3Jijel University, Jijel, Constantine, Algeria; 4Icahn School of Medicine at Mount Sinai, New York, NY; 5Weill Cornell Medicine, New York, NY Introduction: Obesity is a global health issue, and bariatric surgery, especially Roux-en-Y gastric bypass, is a common treatment. The altered anatomy caused by bariatric surgery complicates traditional ERCP. Comparative data on ERCP outcomes, particularly post-ERCP pancreatitis (PEP), in bariatric vs. non-bariatric patients remain limited. This study assesses ERCP safety and adverse event rates in patients with prior bariatric surgery. Methods: We analyzed Nationwide Inpatient Sample data from 2016–2019. Patients undergoing inpatient ERCP were identified via ICD-10 procedural codes. Outcomes included mortality, length of stay (LOS), hospital charges, and adverse events (PEP, bleeding, perforation, infections). Multivariable logistic regression adjusted for demographics, comorbidities, and procedure types to assess PEP risk factors. Analyses were performed using SPSS, with significance set at p< 0.05. Results: The study included 366,700 controls and 4,540 patients with prior bariatric surgery. Bariatric surgery patients were younger (mean age 55.44 vs. 63.14 years, p< 0.001) and predominantly female (76.2% vs. 56.6%, p< 0.001). A higher proportion of bariatric surgery patients were obese (41.7% vs. 16.9%, p< 0.001) and privately insured (44.4% vs. 26.8%, p< 0.001). They had lower Charlson Comorbidity Index scores (p< 0.001) and were more likely to undergo diagnostic ERCP (14.2% vs. 12.6%, p=0.001). Regarding outcomes, bariatric surgery patients had shorter length of stay (4.81 vs. 5.13 days, p< 0.001) and similar total charges (p=0.545). Mortality rates were lower in the bariatric group (0.9% vs. 1.2%, p=0.038), but this was not statistically significant after adjustment (aOR 1.30, 95% CI 0.92–1.82, p=0.135). Bariatric patients had reduced risk of post-ERCP pancreatitis (aOR 0.75, 95% CI 0.60–0.93, p=0.009), while rates of post-ERCP infection, bleeding, and perforation were similar between groups. Discussion: Bariatric patients undergoing ERCP had shorter hospital stays and fewer adverse events, including PEP and infections, compared to non-bariatric controls. Although bariatric surgery independently reduced PEP risk, it did not significantly influence post-ERCP mortality or infections. The protective effect of bariatric surgery against PEP may be attributed to anatomical changes, improved metabolic profiles, and refined perioperative care. Further research is warranted to elucidate the mechanisms and evaluate long-term outcomes in this population.
Figure: Table 1. Comparison of Demographic, Clinical, and Post-ERCP Outcomes Between Bariatric and Non-Bariatric Patients
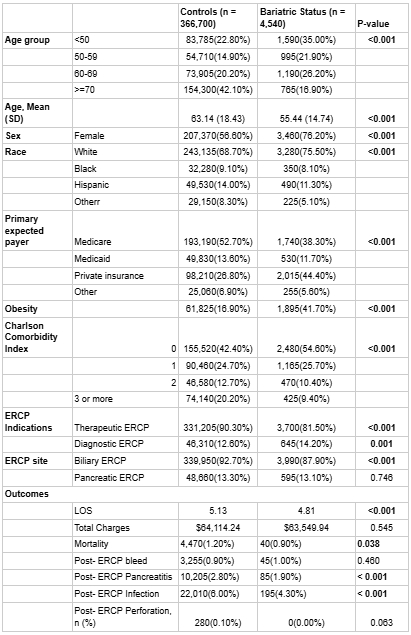
Figure: Figure 1. Adjusted odds ratios (aORs) for post-ERCP outcomes in bariatric vs. non-bariatric patients. Only post-ERCP pancreatitis was significantly reduced in bariatric patients (aOR 0.75, p=0.009).
Disclosures: Sarah Meribout indicated no relevant financial relationships. Ahmed Salem indicated no relevant financial relationships. Anis Meribout indicated no relevant financial relationships. Saida Benmostefa indicated no relevant financial relationships. Ovanes Karslyan indicated no relevant financial relationships. Urmil Shah indicated no relevant financial relationships. Kamal Hassan indicated no relevant financial relationships. Fatima Khan indicated no relevant financial relationships. Nakul Mahajan indicated no relevant financial relationships. Yasutoshi Shiratori indicated no relevant financial relationships.
Sarah Meribout, MD1, Ahmed Salem, MD1, Anis Meribout, MD2, Saida Benmostefa, MS3, Ovanes Karslyan, MD1, Urmil Shah, MD4, Kamal Hassan, MD5, Fatima Khan, MD1, Nakul Mahajan, MBBS1, Yasutoshi Shiratori, MD1. P3520 - Is ERCP Safer in Bariatric Surgery Patients? A Nationwide Analysis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.