P3508 - Comparative Outcomes of Gastrostomy Tube Placement by Gastroenterology vs Interventional Radiology: A Propensity-Matched Analysis of Over 100,000 Patients
University of California Riverside School of Medicine Riverside, CA
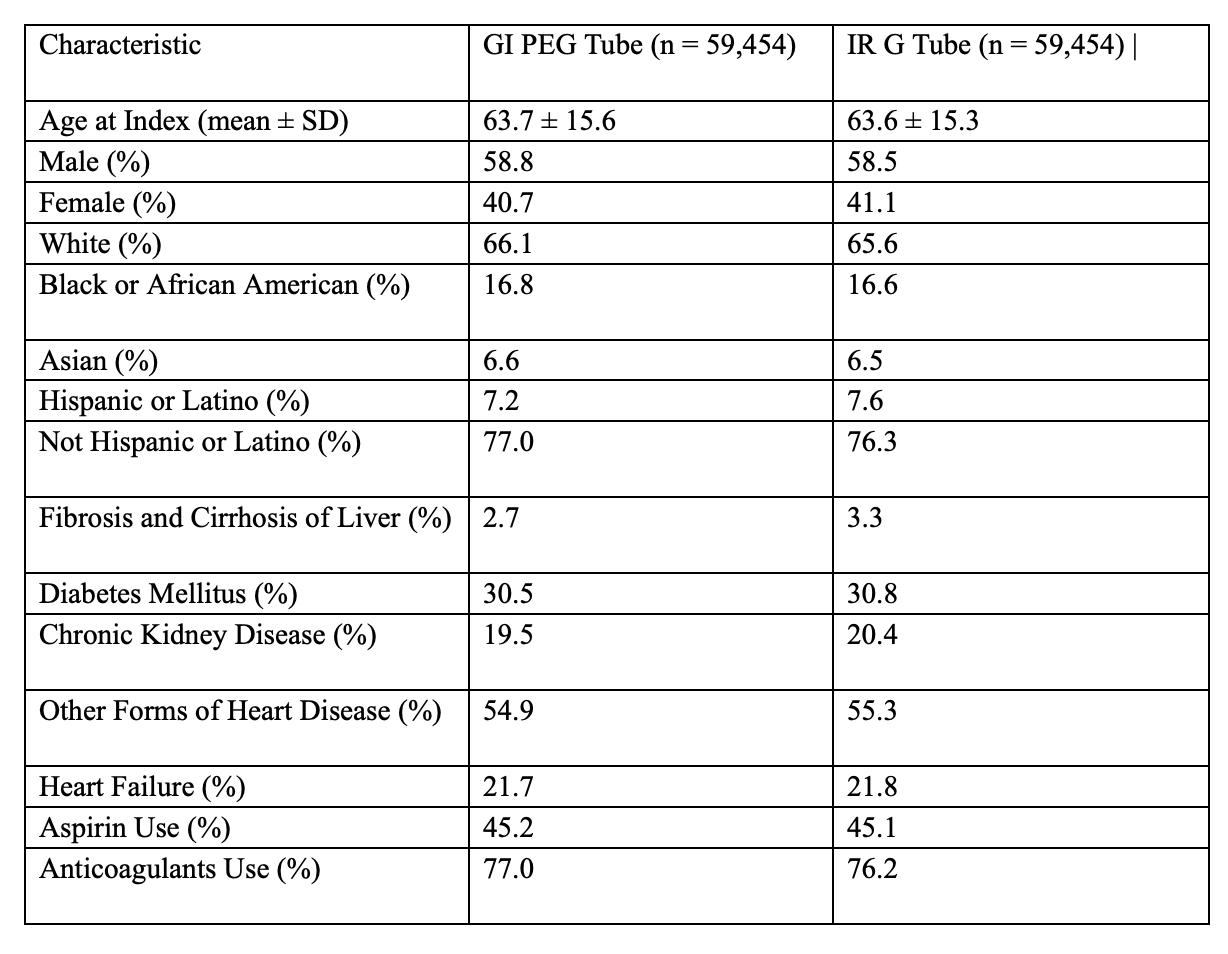
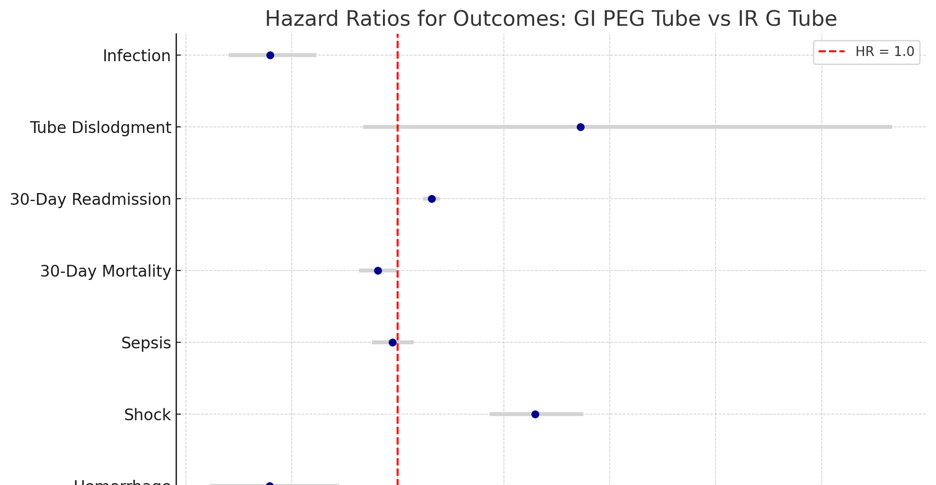
Ashujot K. Dang, MD1, Vikash Kumar, MD2, Fnu Rashmi, MD3, Aalam Sohal, MD2, Pir Shah, MD4, Ariana R. Tagliaferri, MD2, Aida Rezaie, MD2 1University of California Riverside School of Medicine, Riverside, CA; 2Creighton University School of Medicine, Phoenix, AZ; 3University of California Riverside School of Medicine, Redlands, CA; 4Creighton University Medical Center, Phoenix, AZ Introduction: Gastrostomy tubes are routinely placed for long-term enteral nutrition in patients unable to maintain adequate oral intake. There are two ways: percutaneous endoscopic gastrostomy tube by gastroenterology (GI PEG tube) or fluoroscopic placement by interventional radiology (IR G-tube). However, comparative safety and outcome data between the two remain limited. Understanding the relative risks associated with each approach is essential for guiding clinical decision-making, especially in complex or high-risk patients. This study compares short-term outcomes of GI vs IR G-tube placement using real-world data from a large, multi-institutional electronic health record (EMR) network. Methods: We conducted a retrospective cohort study using the TriNetX US Collaborative Network, encompassing EMR from 69 healthcare organizations. We included adults (≥18 yrs) who underwent GI PEG (CPT 43246) with IR G-tube (CPT 49440) techniques between 2005 and 2025 with 30 days post-procedure follow-up. Propensity score matching (PSM) (1:1) was performed to control for baseline demographics, comorbidities (e.g., diabetes, CKD, cirrhosis, heart failure), and relevant medications (Table 1). Primary outcomes included 30-day mortality, hemorrhage, sepsis, infection, tube dislodgement, and 30-day readmission. Risk analyses and Kaplan-Meier survival curves were used to compare outcomes between groups. Results: After PSM, each cohort had 59,454 patients. Interestingly, GI PEG was associated with lower risks of Hemorrhage (0.4% vs 0.6%, OR 0.75); Infection (1.0% vs 1.3%, OR 0.75); 30-day mortality (9.0% vs 9.4%, OR 0.95). However, GI PEG placement was associated with higher risks of 30-day readmission (63.4% vs 59.6%, OR 1.17). Furthermore, there were no significant differences in sepsis (8.1% vs 8.3%, p=0.42) or tube dislodgement (0.1% in both groups, p=0.12) (Figure 1). Discussion: This large, propensity-matched cohort study with over 100,000 patients, GI PEG was associated with lower risks of hemorrhage, infection, and 30-day mortality compared to IR G-tube. However, GI PEG placement had higher rates of 30-day readmission. These findings can help in clinical decision-making and highlight important trade-offs between the two techniques. It underscores the benefit of GI PEG tube placement over IR G tube, with overall better outcomes, while stressing the need for individualized decision-making based on patient risk profiles and institutional expertise.
Figure: Table 1: Baseline Characteristics After Propensity Score Matching
Figure: Hazard ratios of outcomes GI PEG vs IR G tube
Disclosures: Ashujot Dang indicated no relevant financial relationships. Vikash Kumar indicated no relevant financial relationships. Fnu Rashmi indicated no relevant financial relationships. Aalam Sohal indicated no relevant financial relationships. Pir Shah indicated no relevant financial relationships. Ariana Tagliaferri indicated no relevant financial relationships. Aida Rezaie indicated no relevant financial relationships.
Ashujot K. Dang, MD1, Vikash Kumar, MD2, Fnu Rashmi, MD3, Aalam Sohal, MD2, Pir Shah, MD4, Ariana R. Tagliaferri, MD2, Aida Rezaie, MD2. P3508 - Comparative Outcomes of Gastrostomy Tube Placement by Gastroenterology vs Interventional Radiology: A Propensity-Matched Analysis of Over 100,000 Patients, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.