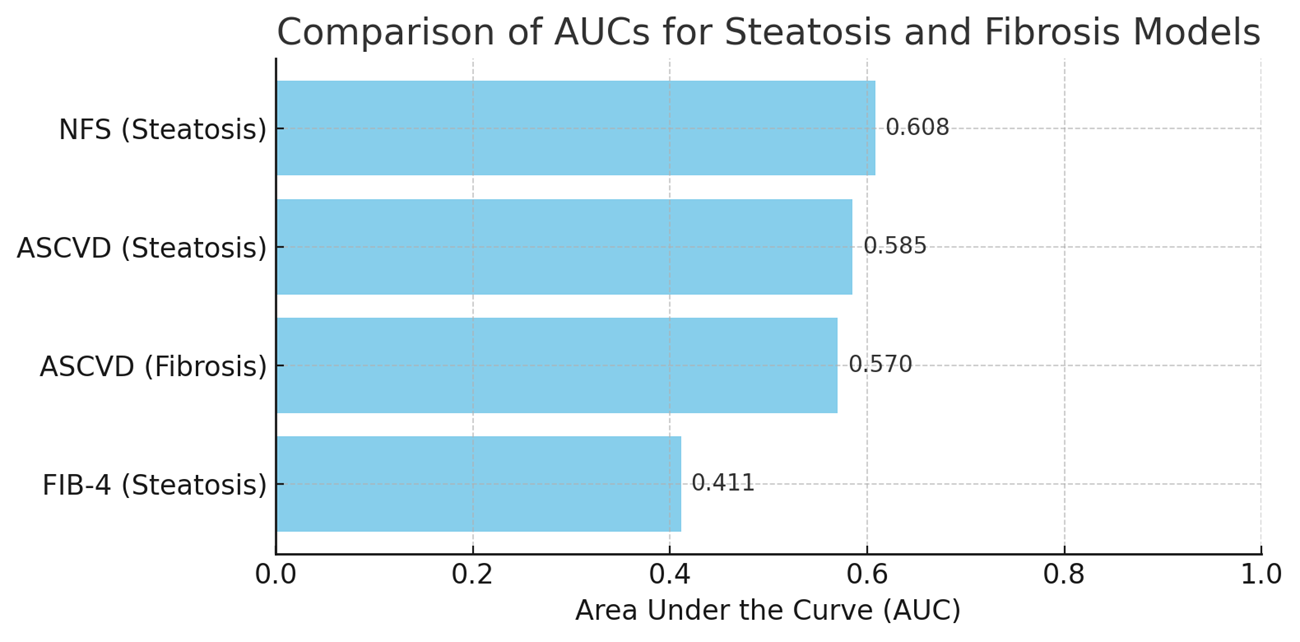
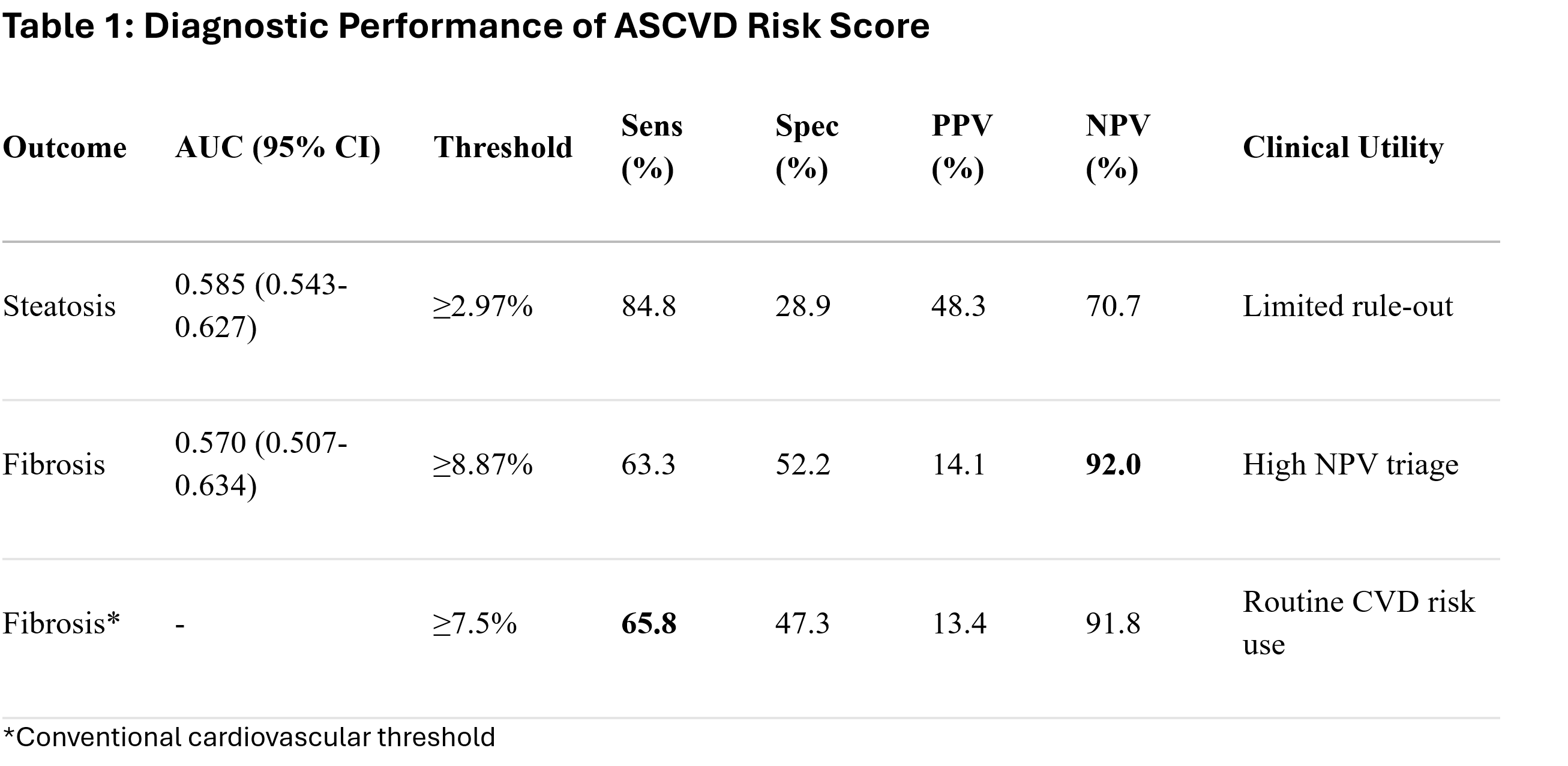
Chukwuemeka Ogbu, MD, MPH1, Ndukwe J. Kalu, MD, MPH2, Oyedotun Babajide, MD3, Lekhya Kollu, BA4, Philip Okafor, MD, MPH, FACG5 1Cape Fear valley Medical Center, Fayetteville, NC; 2Cape Fear Health, Fayetteville, NC; 3NYC Health + Hospitals/Metropolitan, New York, NY; 4Lewis Katz School of Medicine at Temple University, Philadelphia, PA; 5Mayo Clinic, Jacksonville, FL Introduction: Metabolic dysfunction-associated steatotic liver disease (MASLD) and atherosclerotic cardiovascular disease (ASCVD) share overlapping metabolic risk factors, suggesting the potential diagnostic crossover of cardiovascular risk tools for liver disease detection. However, the diagnostic performance of the widely used ASCVD 10-year risk score for hepatic steatosis and fibrosis remains unestablished. Methods: We conducted a cross-sectional analysis of 717 adults from the National Health and Nutrition Examination Survey ( NHANES) 2017–2020 cohort with complete ASCVD risk scores and vibration-controlled transient elastography (VCTE) data. Hepatic steatosis was defined as controlled attenuation parameter (CAP) ≥288 dB/m (moderate-to-severe), and significant fibrosis as liver stiffness measurement (LSM) ≥8.0 kPa. Receiver operating characteristic (ROC) analysis compared ASCVD against FIB-4 and NAFLD Fibrosis Score (NFS). Results: The ASCVD risk score demonstrated poor discrimination for both steatosis (AUC 0.585, 95% CI: 0.543-0.627) and fibrosis (AUC 0.570, 95% CI: 0.507-0.634). While it outperformed FIB-4 (steatosis AUC 0.411; fibrosis AUC < 0.5), ASCVD was inferior to NFS for steatosis detection (AUC 0.608). At optimal thresholds, ASCVD showed high sensitivity but low specificity for steatosis (84.8% and 28.9% at ≥2.97%), and modest performance for fibrosis (63.3% sensitivity, 52.2% specificity at ≥8.87%). Notably, at the conventional ASCVD ≥7.5% threshold used in cardiovascular risk assessment, fibrosis sensitivity was 65.8% with preserved negative predictive value (NPV 91.8%). Risk stratification revealed actionable MASLD prevalence doubled from low-risk (8.8% at ASCVD< 5%) to high-risk groups (13.3% at ASCVD≥15%). Discussion: The ASCVD risk score exhibits inadequate diagnostic accuracy for hepatic steatosis and fibrosis. Its marginal superiority over FIB-4 reflects contextual limitations of existing liver scores rather than intrinsic diagnostic value. While the preserved NPV at routine clinical thresholds may support secondary triage for fibrosis, these findings preclude its use as a primary screening tool for MASLD.
Figure: Diagnostic Performance of ASCVD Risk Score
Figure: Comparisons of AUCs for fibrosis and steatosis models
Disclosures: Chukwuemeka Ogbu indicated no relevant financial relationships. Ndukwe Kalu indicated no relevant financial relationships. Oyedotun Babajide indicated no relevant financial relationships. Lekhya Kollu indicated no relevant financial relationships. Philip Okafor indicated no relevant financial relationships.
Chukwuemeka Ogbu, MD, MPH1, Ndukwe J. Kalu, MD, MPH2, Oyedotun Babajide, MD3, Lekhya Kollu, BA4, Philip Okafor, MD, MPH, FACG5. P3679 - ASCVD Risk Score Demonstrates Limited Diagnostic Utility for Hepatic Steatosis and Fibrosis in a Nationally Representative Sample, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.