North Shore University Hospital - Northwell Health Manhasset, NY
Jade Pace, MD, Ajay Jassal, MD, Annamaria Iakovou, MD North Shore University Hospital - Northwell Health, Manhasset, NY Introduction: Acute pulmonary edema is an unrecognized, but life-threatening complication of paracentesis. To date, only two cases have been reported in the literature.1,2 We present a case of a male with cirrhosis developing pulmonary edema after first-time paracentesis.
Case Description/
Methods: A 59-year-old male with recent diagnosis of cirrhosis, alcohol use disorder, and hypertension presented to the Emergency Department for decompensated cirrhosis with first episode of ascites. Interventional Radiology performed a paracentesis on a large fluid pocket found in the right upper quadrant (Figure 1). The procedure was initiated without complications and with stable vitals. However, after drainage of 10.3 liters of clear yellow fluid, the patient developed acute dyspnea, hypoxemia, and hypotension to blood pressures of 80s/50s refractory to albumin and 1 liter of normal saline.
Chest x-ray and Computed Tomography were significant for bilateral patchy airspace opacities suggestive of asymmetric pulmonary edema (Figure 2). Patient was placed on high flow nasal cannula and given diuresis with furosemide 40mg daily and spironolactone 100mg twice a day. After several days of diuretics and albumin, the patient was gradually able to be weaned to room air. Blood pressure also stabilized during this time. An echocardiogram during this admission was unremarkable with an ejection fraction of 71% and normal diastolic function. Creatinine was within normal range. One week after discharge, the remainder of ascitic fluid (9 liters) was removed by repeat paracentesis without any complications. Discussion: This case represents an unusual complication of an otherwise standard procedure, irrespective of proceduralist ability. The pathophysiology is unclear, but we hypothesize that the ventricles were unable to accommodate the rapid increase of preload secondary to the decrease in abdominal pressure. There may also be a physiological response alluding to tolerance as our patient’s subsequent paracenteses were uneventful, like prior.1 We bring attention to this unpredictable and rare outcome to highlight the importance of clinical diligence in performing paracenteses.
1. Holbert et al, A Case of Reexpansion Pulmonary Edema Following Large Volume Paracentesis, m J Respir Crit Care Med, 2022, 205: A4196.
2. Sharma A, Fletcher A, Lipscomb GR, Pulmonary oedema after therapeutic ascitic paracentesis: a case report and literature review of the cardiac complications of cirrhosis, Eur J Gastroenterol Hepatol, 2010 Feb, 22(2): 241-5.
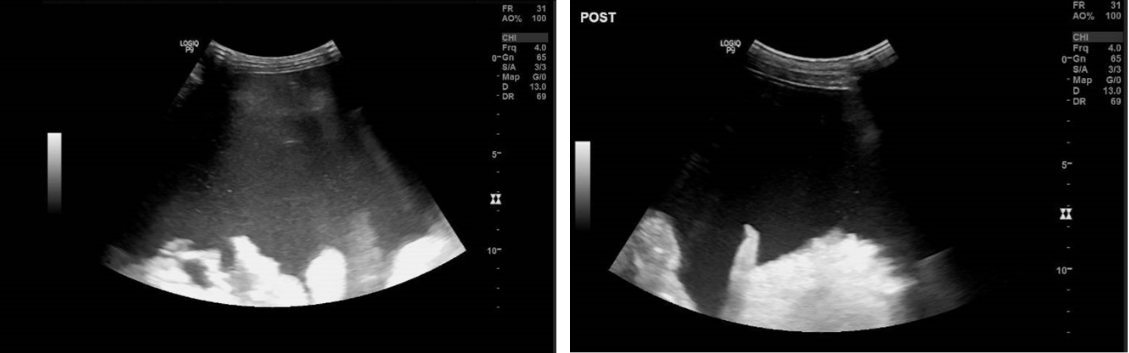
Figure: Figure 1. Ultrasound of abdomen demonstrating large fluid pocket in right upper quadrant pre-paracentesis (left) and post-paracentesis (right).
Disclosures: Jade Pace indicated no relevant financial relationships. Ajay Jassal indicated no relevant financial relationships. Annamaria Iakovou indicated no relevant financial relationships.
Jade Pace, MD, Ajay Jassal, MD, Annamaria Iakovou, MD. P6110 - Acute Pulmonary Edema Elicited by Initial Paracentesis in New Cirrhosis: A Case Report, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")