University of Texas Health San Antonio San Antonio, TX
Cody Hu, MD, Neha Sharma, MD, Naga Vura, MD University of Texas Health San Antonio, San Antonio, TX Introduction: Abdominal wall varices are a cluster of distended and engorged veins across the abdomen. Here, we report a case of abdominal wall variceal bleeding and its management in a patient with cirrhosis and portal hypertension.
Case Description/
Methods: A 57-year-old male with alcoholic cirrhosis was admitted for active hemorrhage from his anterior abdominal wall. Vitals showed tachycardia and hypertension. Physical exam revealed a distended abdomen with a ventral hernia that was associated with a pool of blood (Image 1). Initial Hgb level was low at 5.3 g/dL, and it only stabilized at 7.6 g/dL after a 4-unit blood transfusion. CT of the abdomen revealed extensive varices in the ventral abdominal wall (Image 2). Subsequent CT angiogram confirmed increased contrast opacification within the conglomerated varices at the ventral hernia, which was reflective of venous bleeding. Multiple figure-of-8 stitches were placed over the varix by the surgical team to control bleeding. TIPS was urgently done with IR to reduce portal hypertension and bleeding. He was discharged home with propranolol after bleeding was controlled. However, three days later, the patient presented back to the ER for active bleeding from his midline periumbilical insertion site. The patient was brought to the operating room emergently for percutaneous embolization of the inflow section from the umbilical vein. His bleeding was stopped entirely over the next few days. Discussion: Variceal bleeding is a common complication of cirrhosis and portal hypertension. It carries a 10% to 20% mortality rate in the 6 weeks following the variceal rupture. The managements of abdominal wall varices are not commonly reported in the existing literature. It is intuitive to suspect that abdominal wall varices are superficial and readily viewed on physical exam. However, these varices can also be subtle and buried under the skin and adipose tissue, as our patient presented. A CT angiogram was used in our patient, and this modality can both detect abdominal wall varices and differentiate between venous and arterial bleeding. Surgical intervention with suture ligation functioned as a bridge for him to have TIPS placement. Unfortunately, TIPS failed to control his variceal bleeding despite adequate blood flow in the shunt. Percutaneous embolization of his umbilical vein was done as a complementary approach to TIPS. This case highlights the managements of acute external variceal hemorrhage, and surgical ligation allows rapid and direct control of bleeding vessels.
Figure: Image 1. Variceal bleeding at ventral hernia.
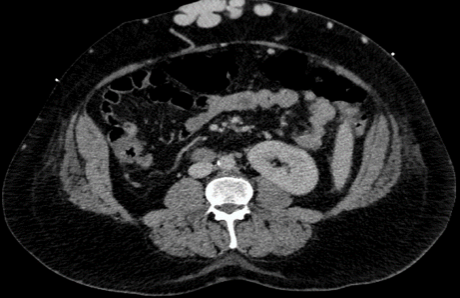
Figure: Image 2. Extensive varices identified along the ventral abdominal wall soft tissues with a dilated varix seen extending to the cutaneous surface, likely representing serosal bleeding on CT scan.
Disclosures: Cody Hu indicated no relevant financial relationships. Neha Sharma indicated no relevant financial relationships. Naga Vura indicated no relevant financial relationships.
Cody Hu, MD, Neha Sharma, MD, Naga Vura, MD. P6102 - When Portal Hypertension Strikes the Surface: A Case of Life-Threatening Abdominal Wall Variceal Bleeding, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.