Section of Gastroenterology and Hepatology, Dartmouth-Hitchcock Medical Center Lebanon, NH
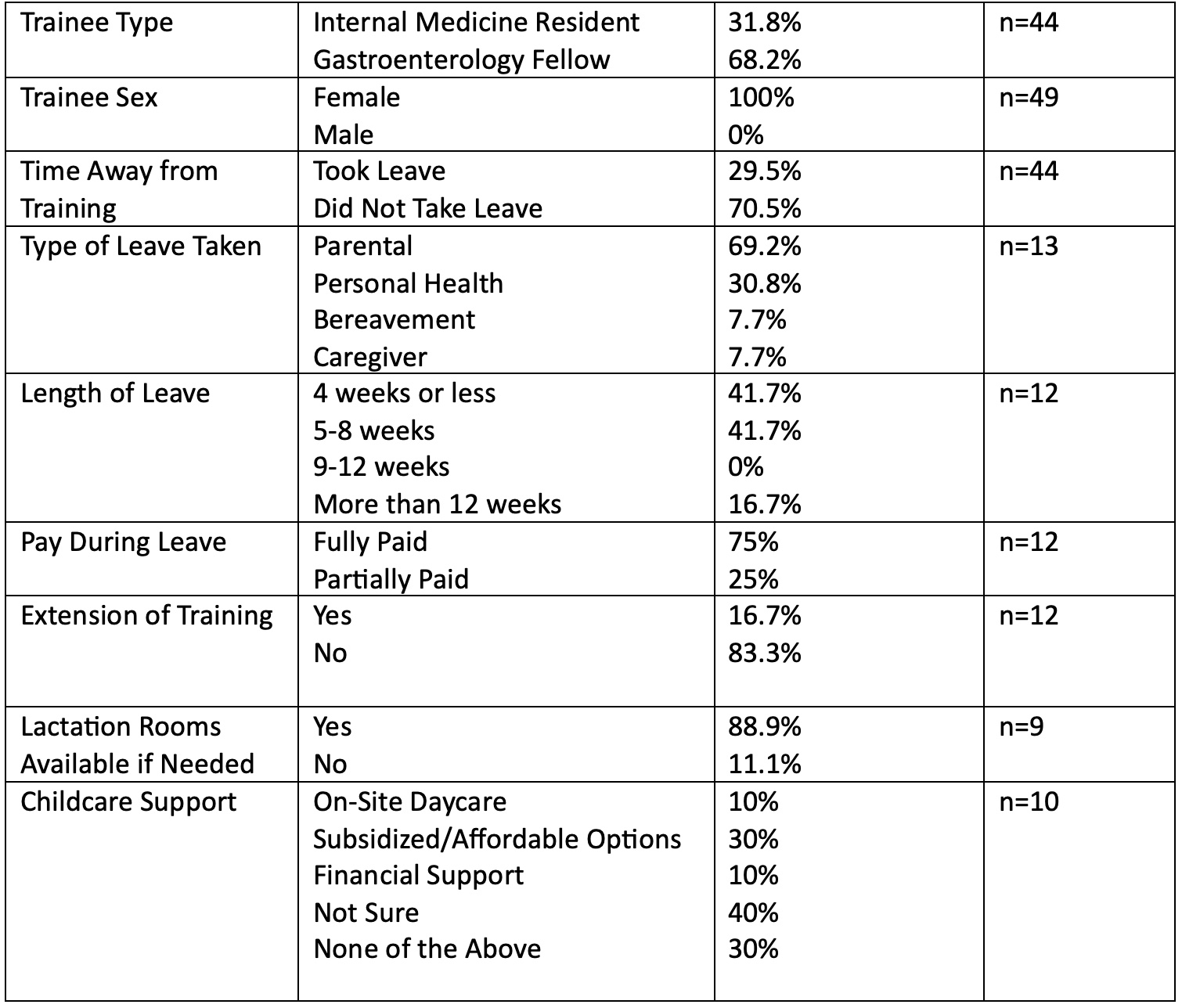
Jamie M. Horrigan, MD1, Aimen Farooq, MD2, Lauren Feld, MD3, Anita Afzali, MD, MPH, MHCM4, Aline Charabaty, MD, FACG5 1Section of Gastroenterology and Hepatology, Dartmouth-Hitchcock Medical Center, Lebanon, NH; 2Department of Gastroenterology and Hepatology, AdventHealth Orlando, Orlando, FL; 3University of Massachusetts Chan School of Medicine, Worcester, MA; 4Department of Internal Medicine, Division of Digestive Diseases, University of Cincinnati College of Medicine, Cincinnati, OH, USA, Cincinnati, OH; 5Johns Hopkins University School of Medicine, Washington, DC Introduction: Fair, transparent, and well-communicated parental leave policies have been shown to be important for recruiting, retaining, and supporting gastroenterology (GI) trainees. However, many face uncertainty, stigma, and systemic barriers when navigating leave during training. Previous studies have identified that women in particular report being dissuaded from GI fellowship due to concerns about lack of parental leave. This study evaluated trainees’ knowledge of leave policies, their experiences taking leave, and the impact of a targeted educational intervention. Methods: At the 2025 Scrubs & Heels Leadership Summit, a trainee-focused session addressed navigating parental leave during training. Prior to the session, trainees completed a survey assessing awareness of institutional and Accreditation Council for Graduate Medical Education (ACGME) leave policies, and prior leave experiences. The interactive session covered ACGME, institutional, and state policies, Family & Medical Leave Act, short-term disability, board eligibility, and practical negotiation strategies. Post-session surveys measured changes in knowledge, comfort, and preparedness. Results: 49 female trainees attended with 89.8 and 81.6% pre- and post-survey response rates (Table 1). At baseline, 50% were unaware of institutional or ACGME leave policies. 50% expressed discomfort discussing parental leave with program leadership. Barriers to taking leave included workload redistribution (37%), burdening peers (22%), and training extension (22%). 29.5% took leave during training, of which 40% felt taking leave negatively impacted performance evaluations. There was wide variation in call coverage. Most found returning to work challenging, and most did not receive schedule accommodations (Figure 1). Following the session, over 95% demonstrated improved understanding of leave policies and board eligibility, 82.5% felt more comfortable discussing leave policies and negotiating schedules, and 97.5.% would recommend the session to other trainees. Discussion: GI trainees face substantial gaps in knowledge, support, and communication regarding parental leave. Many fear stigma, logistical burdens, and adverse career impacts. This session greatly improved awareness and self-efficacy in navigating leave. Institutions must develop transparent, equitable, and trainee-centered leave policies to foster an inclusive training environment, support work-life integration, and ensure equitable advancement for all future parents and caregivers.
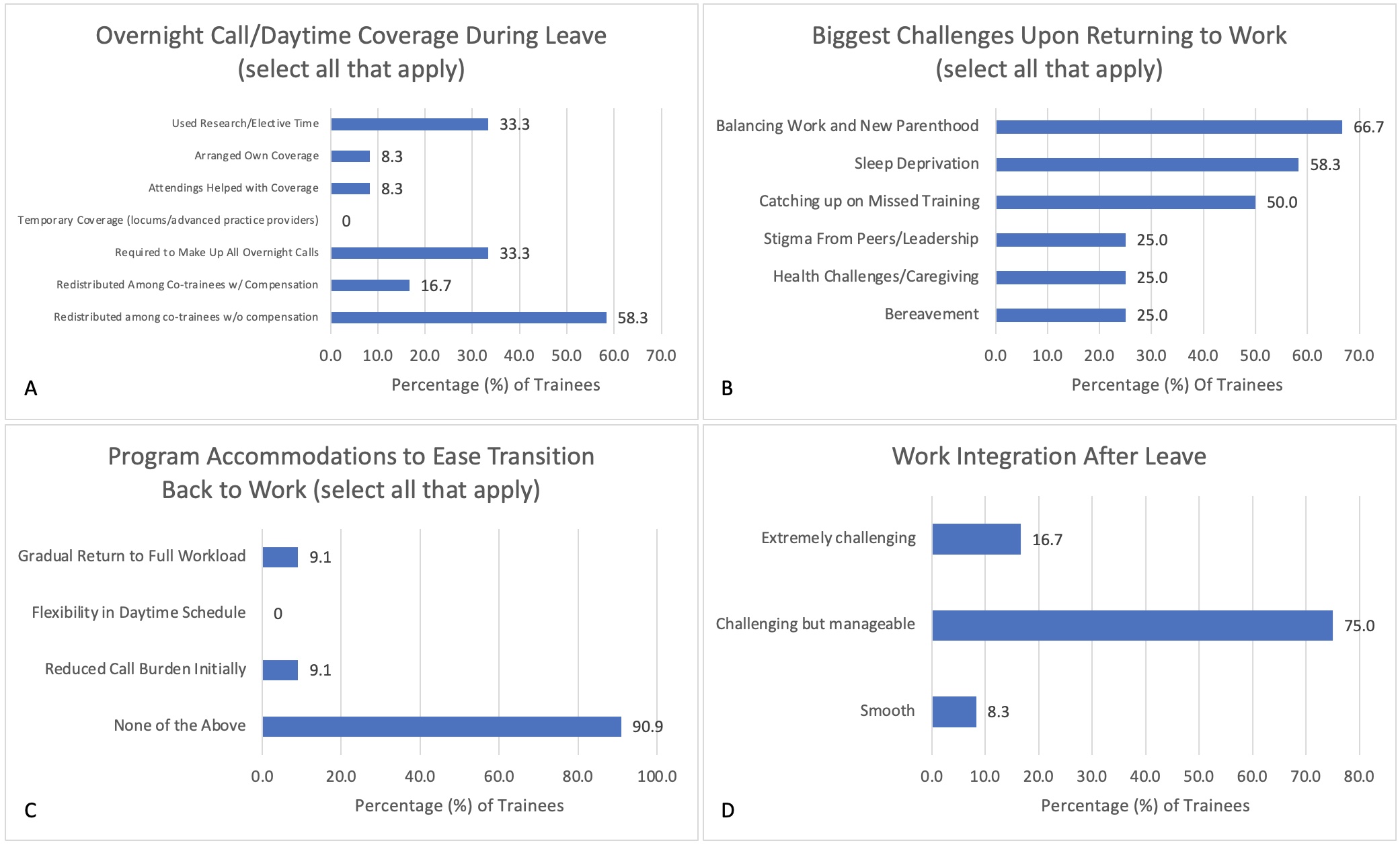
Figure: Figure 1. Internal medicine and gastroenterology trainees who have taken time away from training were asked about (A) Overnight call/daytime coverage during leave, (B) biggest challenges upon returning to work, (C) program accommodations to ease the transition back to work, and (D) the ease of integrating back into work after leave.
Figure: Table 1. Characterizing Time Away From Training in a Cohort of Internal Medicine/GI Trainees