University of Connecticut Health Center Farmington, CT
Danzhu Zhao, DO1, Neil Khoury, MD1, Osama Siddique, MD2 1University of Connecticut Health Center, Farmington, CT; 2Connecticut GI, Wallingford, CT Introduction: Follicular lymphomas (FL) are often indolent and rarely affect the gastrointestinal (GI) tract. When it does involve the GI tract, it most often affects the small bowel. FLs can transform histologically to diffuse large B- cell lymphoma (DLBCL) years after initial diagnosis. We present a case that highlights the importance of having a high index of suspicion for intra-abdominal lymphomas in patients with abdominal pain and a prior history of lymphoma without classic “B” symptoms such as fevers, night sweats and weight loss.
Case Description/
Methods: A 71-year-old male with a history of FL with small bowel involvement status post appendectomy, ileocecectomy and chemotherapy, presented with five days of worsening abdominal pain, nausea, and vomiting. He denied fevers, chills, unintentional weight loss or change in bowel habits.
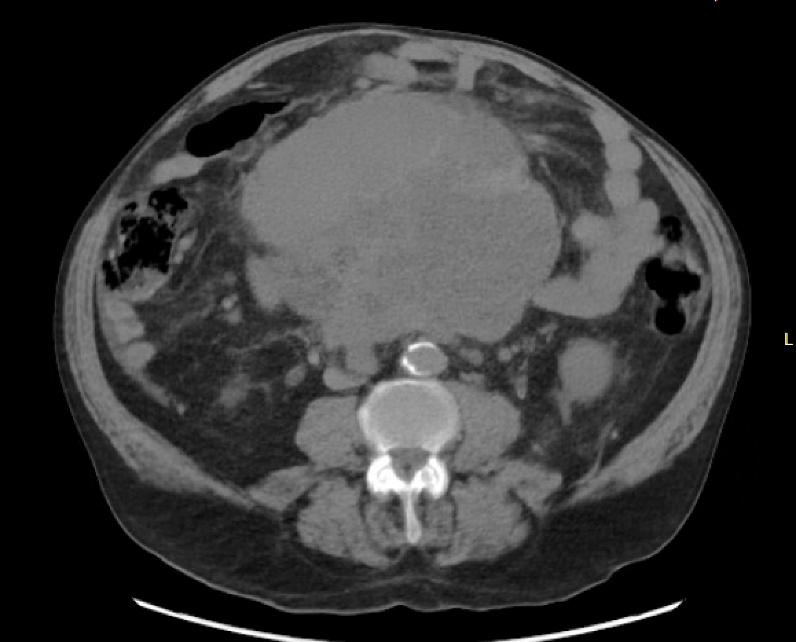
On exam, he was hypertensive and had abdominal distension with lower abdominal tenderness. Laboratory studies were normal. A six-month prior PET CT scan showed mesenteric soft tissue heterogeneity with two small foci of increased uptake. CT abdomen/pelvis this presentation revealed a 14.6 x 16.5 x 16 cm confluent central mesenteric mass with encasement of central mesenteric vasculature and the duodenum (Figure 1) with mesenteric and retroperitoneal lymphadenopathy. Percutaneous sampling was not feasible due to overlying bowel and mesenteric vasculature. Endoscopic ultrasound (EUS) revealed many enlarged perigastric and peripancreatic lymph nodes. Fine needle biopsy of lymph nodes (Figure 2) demonstrated monoclonal B-cell non-Hodgkin lymphoma. The patient was started on prednisone with improvement of his abdominal pain and was initiated on chemotherapy with close oncology follow-up. Discussion: Intestinal FLs are often indolent for years and can lack “B” symptoms. Despite prior surgery and chemotherapy, our patient presented with acute GI symptoms from a large mesenteric mass with biopsy suggestive of DLBCL transformation. The most common extra nodal site often involves the GI tract and can also present without “B” symptoms. Our case demonstrates the need for a high index of suspicion for FL transformation to DLBCL post-treatment, particularly in patients without “B” symptoms or hematologic abnormalities. EUS proved invaluable in safely obtaining biopsies for histopathologic confirmation particularly when percutaneous biopsies are not feasible. The patient’s abdominal symptoms improved with steroids and was ultimately initiated on chemotherapy.
Figure: Figure 1. CT abdomen/pelvis revealed a 14.6 x 16.5 x 16 cm confluent central mesenteric mass with encasement of central mesenteric vasculature and the duodenum.
Figure: Figure 2. Fine needle biopsy of perigastric and peripancreatic lymph nodes during endoscopic ultrasound.
Disclosures: Danzhu Zhao indicated no relevant financial relationships. Neil Khoury indicated no relevant financial relationships. Osama Siddique indicated no relevant financial relationships.
Danzhu Zhao, DO1, Neil Khoury, MD1, Osama Siddique, MD2. P6260 - Silent Progression: Intra-Abdominal B-Cell Lymphoma in the Absence of Systemic Symptoms, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.