Yeshika Thapa, MD1, Bahar Rehan, MD2, Saar Pales, MBBS3, Bellal Alfar, MD4, Mohammad Abuassi, MD2, Aiman Obed, MD, PhD4 1University of Central Florida, Gainesville, FL; 2University of Central Florida, HCA Healthcare GME, Gainesville, FL; 3University of Central Florida College of Medicine, Orlando, FL; 4Ibn Sina University for Medical Sciences, Amman, 'Amman, Jordan Introduction: Neuroendocrine tumors (NETs) of the gastrointestinal tract can clinically and radiologically resemble inflammatory bowel diseases like Crohn’s, often leading to delayed or incorrect diagnoses. This case illustrates how persistent gastrointestinal symptoms unresponsive to standard therapy should prompt re-evaluation and consideration of alternative diagnoses.
Case Description/
Methods: A 56-year-old woman presented with a 10-month history of colicky abdominal pain, diarrhea, vomiting, and significant weight loss. She was initially diagnosed with Crohn’s disease and received corticosteroids, azathioprine, and later adalimumab, without lasting clinical benefit. Imaging revealed ileal wall thickening, luminal narrowing, and a suspicious soft-tissue mass in the terminal ileum. Due to persistent symptoms and worrisome imaging, she underwent mini-laparotomy and ileal resection. Histopathological analysis confirmed a 1.5 cm, Grade 1 well-differentiated neuroendocrine tumor (pT4 pN1), with lymphovascular and perineural invasion. Six of twelve regional lymph nodes were positive for metastasis. Postoperative recovery was uneventful, and the patient was referred to oncology for further management. Discussion: This case report discusses the diagnostic challenge posed by ileal NETs mimicking Crohn’s disease. The overlap in clinical symptoms and imaging findings can obscure accurate diagnosis, particularly in patients with refractory symptoms. Timely surgical evaluation and histopathologic confirmation were crucial in this case. Clinicians should maintain a broad differential when standard therapies fail, as misdiagnosis can delay appropriate oncologic care and adversely impact prognosis.
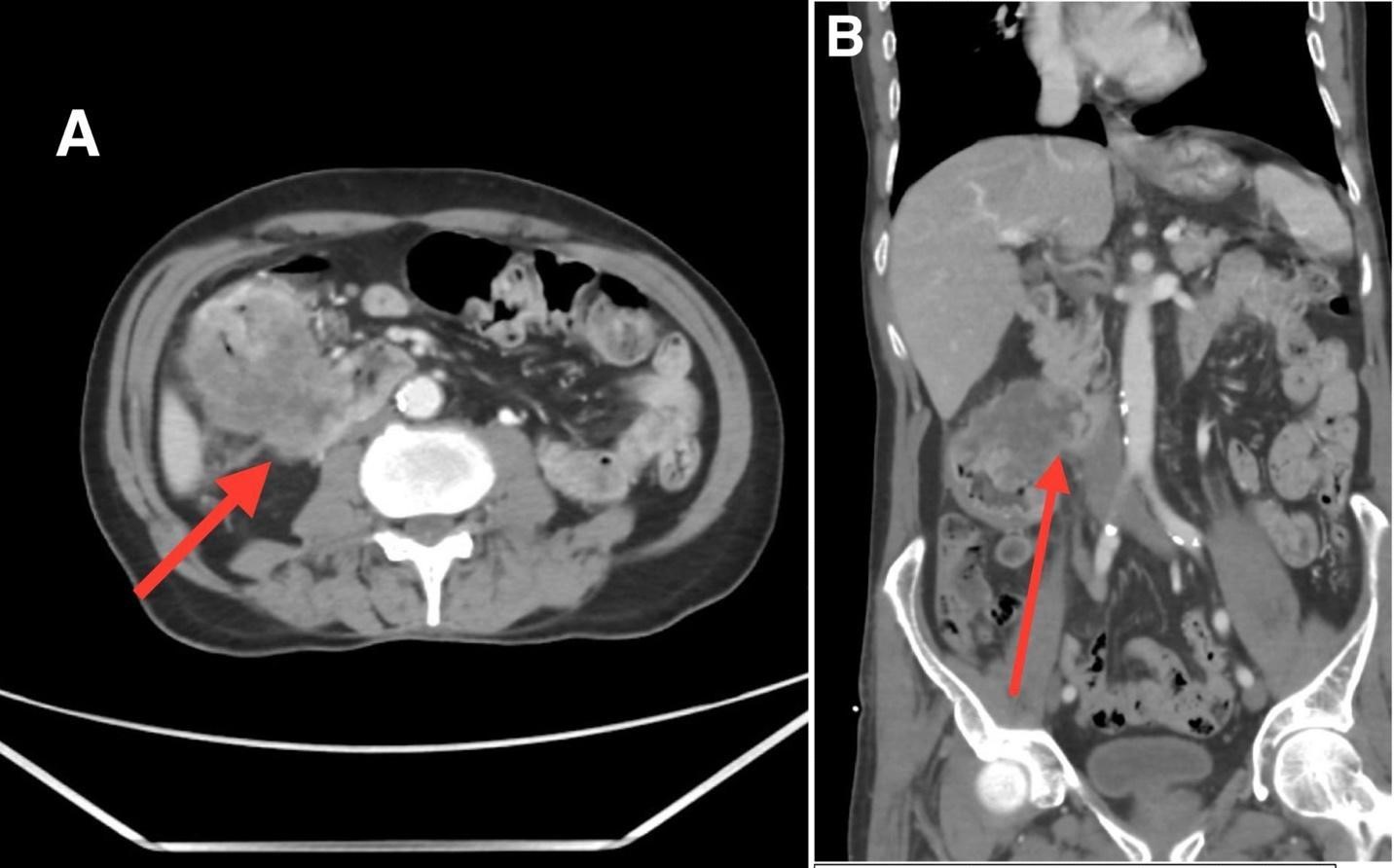
Figure: Contrast-enhanced axial (A) and coronal (B) computed tomography images showing a soft-tissue mass (red arrows) in the terminal ileum with associated bowel wall thickening and luminal narrowing.
Figure: Intraoperative image showing the terminal ileum with a focal area of stricture and thickening (indicated by the surgeon's hand), corresponding to the site of the neuroendocrine tumor.
Disclosures: Yeshika Thapa indicated no relevant financial relationships. Bahar Rehan indicated no relevant financial relationships. Saar Pales indicated no relevant financial relationships. Bellal Alfar indicated no relevant financial relationships. Mohammad Abuassi indicated no relevant financial relationships. Aiman Obed indicated no relevant financial relationships.
Yeshika Thapa, MD1, Bahar Rehan, MD2, Saar Pales, MBBS3, Bellal Alfar, MD4, Mohammad Abuassi, MD2, Aiman Obed, MD, PhD4. P6248 - Neuroendocrine Tumor of the Terminal Ileum Presenting as Refractory Crohn’s Disease: A Diagnostic Challenge, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.