Varun Chahal, DO1, Marisa Pope, DO2, Yareen Trabelsi, MS3, Edward Bley, DO2, Seth Lipshutz, DO2, Joann Ha, DO4, Nikhitha Mantri, MD4 1Jefferson Health, Stratford, NJ; 2Jefferson Health, Sewell, NJ; 3Rowan-Virtua School of Osteopathic Medicine, Stratford, NJ; 4Jefferson Health, Cherry Hill, NJ Introduction: Gastrointestinal stromal tumors (GISTs) are rare mesenchymal tumors, representing 1–2% of all gastrointestinal neoplasms. While often asymptomatic, GISTs may present with vague symptoms including abdominal pain, melena, hematemesis, or anorexia. We present the case of a 69-year-old male admitted for severe iron deficiency anemia, incidentally found to have a large periduodenal mass with fistulization into the duodenal bulb.
Case Description/
Methods: A 69-year-old male was admitted for evaluation of severe iron deficiency anemia found on outpatient labs. He denied overt GI symptoms aside from generalized fatigue. Medical history included diabetes, hypertension and prostate cancer.
On admission, vitals were stable and physical exam was unremarkable. Labs revealed a hemoglobin of 6.1 g/dL. Contrast-enhanced CT abdomen/pelvis showed a 14.3 × 10.4 × 13.8 cm exophytic duodenal mass with central necrosis and air-fluid level, communicating with the duodenal lumen. The mass also caused extrinsic compression of the common bile duct, resulting in mild intrahepatic biliary dilation.
An esophagogastroduodenoscopy revealed a large ulcerated lesion in the duodenal bulb, initially concerning for a large diverticulum versus a mass. Biopsies showed peptic duodenitis with ulceration and chronic inflammation. Endoscopic ultrasound-guided fine needle aspiration identified a large perigastric and periduodenal mass with fistulization into the duodenum. Histopathology confirmed a gastrointestinal stromal tumor (GIST), with spindle cells positive for DOG-1 and C-KIT and negative for S100 and SMA.
The patient was referred to a tertiary center, where surgery revealed a 14 cm duodenal mass and a 1 cm gastric lesion suggestive of metastasis. Tumor invasion into the liver and encasement of the right hepatic artery rendered it unresectable, so a palliative loop retrocolic isoperistaltic gastrojejunostomy was performed to bypass the obstruction.
He was initiated on neoadjuvant imatinib to downstage the tumor with plans for potential re-evaluation for resection, and continues under close outpatient oncology follow-up. Discussion: Though rare, GISTs should be considered in the differential for GI and hepatobiliary tract masses. Fistulization, while uncommon, may occur silently and complicate the clinical picture. Greater understanding of GIST-associated fistulas is needed to guide further management.
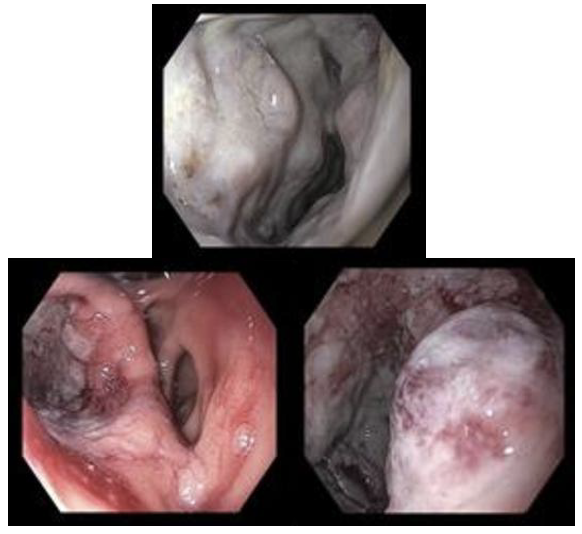
Figure: Figure 1, 2 and 3. Large excavated ulcerated fistula was found in the duodenal bulb. The lesion was friable. The endoscope could not be traversed beyond the lesion.
Disclosures: Varun Chahal indicated no relevant financial relationships. Marisa Pope indicated no relevant financial relationships. Yareen Trabelsi indicated no relevant financial relationships. Edward Bley indicated no relevant financial relationships. Seth Lipshutz indicated no relevant financial relationships. Joann Ha indicated no relevant financial relationships. Nikhitha Mantri indicated no relevant financial relationships.
Varun Chahal, DO1, Marisa Pope, DO2, Yareen Trabelsi, MS3, Edward Bley, DO2, Seth Lipshutz, DO2, Joann Ha, DO4, Nikhitha Mantri, MD4. P6240 - Fistulizing Duodenal GIST Masquerading as a Large Duodenal Diverticulum, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.