John Damianos, MD, Katherine S. King, MS, Alex Lee, BS, Imad Absah, MD, Joseph Murray, MD, Adam C. Bledsoe, MD Mayo Clinic, Rochester, MN Introduction: Celiac disease (CD) causes damage to intestinal villi. Due to co-localization of disaccharidases, CD can result in carbohydrate malabsorption (CM) due to reduced activity of carbohydrate-metabolizing enzymes. Methods: Patients who had undergone testing for CM were screened via ICD codes and confirmed manually for CD by characteristic serologic and histologic findings. Testing modalities included lactose and/or fructose breath tests (BT) and disaccharidase activity assay (via endoscopic biopsy from the duodenum). Positive BT were defined as a rise in breath hydrogen from baseline of ≥20 ppm or a methane level of ≥ 10 ppm at any time. The following cutoffs were used for the disaccharidase assay: lactase < 14, maltase < 70, palatinase < 6, sucrase < 19 and glucoamylase < 8. Marsh score was obtained from the same endoscopy for the disaccharidase biopsies and from an endoscopy within 90 days of BT. Small intestinal bacterial overgrowth (SIBO) testing (BT or aspirate culture) within 30 days of disaccharidase testing was also obtained. Results: We identified 77 patients who had undergone BT (median 37.8 years, interquartile range [IQR] 23-47, 74% female, 98.7% white). Testing occurred within 6 months of diagnosis in 5 (6.5%), 1.6 months-3 years after diagnosis in 3 (3.9%), and >3 years after diagnosis in 69 (89.6%). Fructose BT were positive in 27/58 (46.6%) and lactose in 13/28 (46.4%). There was no association between a positive carbohydrate BT with a positive SIBO test (n tested=45) nor with Marsh score ≥2 (n tested=46) (p = 0.88).
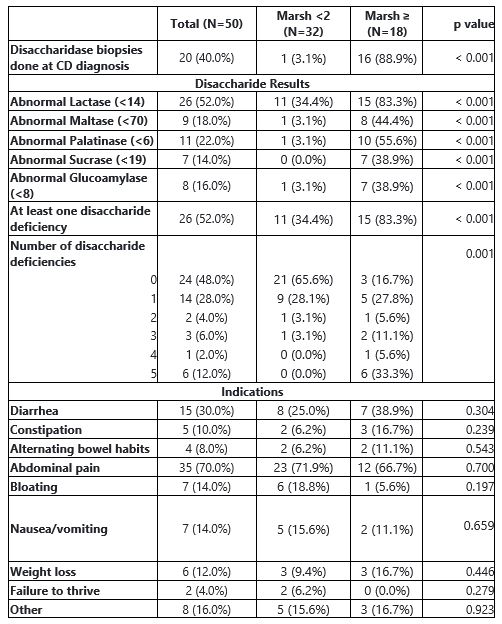
We identified 51 patients who had undergone EGD with biopsies for disaccharidase assay (median age 17.5 years, IQR 15-34, 82.4% female, 94.1% white). Indications are shown in table 1. At least 1 deficiency was seen in 27 (52.9%); abnormal tests by enzyme are displayed in table 1. Marsh score distribution was 0 (27, 54%), 1 (5, 10%), 2 (0, 0%), 3a (11, 22%), 3b (2, 4%), and 3c (5, 10%). Seventeen (33.3%) of the disaccharidase deficiency assays were done at the time of CD diagnosis. Higher Marsh score was significantly associated with the presence of at least 1 disaccharidase deficiency and deficiency of each individual enzyme (table 1). Discussion: CM is common in active CD. Abnormal BT were seen in 46.5% and abnormal disaccharidase assay in 52.9%. Mucosal damage from active CD is associated with reduced activity of all disaccharidases on biopsy. The presence of CM should prompt further investigation for active CD.
Figure: Table 1: Indications for and results of disaccharidase enzyme activity assay and association with Marsh score, comparing Marsh <2 and Marsh ≥2.
Disclosures: John Damianos: ExeGi Pharma – Consultant, Grant/Research Support. i-Health – Speakers Bureau. Katherine King indicated no relevant financial relationships. Alex Lee indicated no relevant financial relationships. Imad Absah indicated no relevant financial relationships. Joseph Murray indicated no relevant financial relationships. Adam Bledsoe: Anokion/Kanyos Bio – Grant/Research Support. Barinthus Bio – Grant/Research Support. Chugai Pharma – Grant/Research Support. Sanofi – Grant/Research Support. Takeda – Grant/Research Support.
John Damianos, MD, Katherine S. King, MS, Alex Lee, BS, Imad Absah, MD, Joseph Murray, MD, Adam C. Bledsoe, MD. P6213 - Carbohydrate Malabsorption Is Common in Active Celiac Disease, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.