The Wright Center for Graduate Medical Education Scranton, PA
Keerthy Gopalakrishnan, MD1, Himani Mongia, MBBS1, Amit Sohagia, MD2 1The Wright Center for Graduate Medical Education, Scranton, PA; 2Geisinger Community Medical Center, Scranton, PA Introduction: Primary duodenal adenocarcinoma (DA) is an uncommon malignancy, representing less than 1% of all gastrointestinal tumors and 0.6% of new cancer diagnoses in the U.S. annually. It often presents with nonspecific gastrointestinal symptoms, contributing to delayed diagnosis and poor prognosis. Peritoneal carcinomatosis is a rare presentation of DA, more commonly associated with ovarian, gastric, or colorectal cancers.
Case Description/
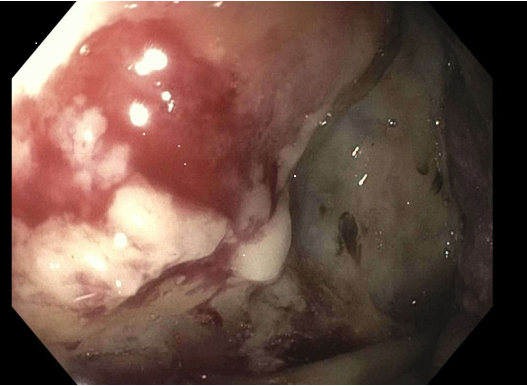
Methods: A 65-year-old male with congestive heart failure, atrial fibrillation, and hypertension presented with a 3-day history of constipation and scant black stools, unrelieved by standard laxatives and enemas. He denied abdominal pain, nausea, or vomiting. Physical examination revealed a distended abdomen with positive fluid thrill. Laboratory studies showed hemoglobin of 7.1 g/dL, elevated alkaline phosphatase (408 U/L), and acute kidney injury. CT imaging revealed large-volume ascites and diffuse omental nodularity concerning peritoneal carcinomatosis, along with a 2 cm hepatic lesion. Paracentesis revealed atypical malignant cells positive for BerEP4, MOC-31, S100P, and CK19. Esophagogastroduodenoscopy revealed a 4 cm circumferential malignant tumor in the third part of the duodenum(Figure 1). Biopsy confirmed moderately differentiated adenocarcinoma with CK7, MUC5AC, and CDX2 positivity. Tumor markers were markedly elevated: CA 19-9 >10,000 U/mL, CEA 28.7 ng/mL, chromogranin A 1531 ng/mL, β-hCG 135.9 mIU/mL. Due to worsening ascites, the patient underwent weekly therapeutic paracenteses. He was later readmitted with spontaneous bacterial peritonitis and gastric outlet obstruction. Attempted duodenal stenting failed due to necrosis and angulation. His condition deteriorated with progressive renal failure, and was transitioned to comfort care. Discussion: This case highlights a rare and aggressive presentation of primary DA with peritoneal carcinomatosis. Literature on such presentations is sparse, with only few case reports describing peritoneal metastasis from small bowel adenocarcinoma. Poor prognostic features included duodenal primary, elevated CA 19-9/CEA, and comorbidities. Our case adds to evidence base and emphasizes the importance of early endoscopic evaluation in patients with ascites and suspected malignancy. Clinicians should maintain a high index of suspicion for small bowel neoplasms in patients with non-specific GI symptoms. Early recognition may facilitate timely palliative intervention and improve quality of life in this aggressive disease.
Figure: Figure 1: Endoscopic image of third part of duodenum
Disclosures: Keerthy Gopalakrishnan indicated no relevant financial relationships. Himani Mongia indicated no relevant financial relationships. Amit Sohagia indicated no relevant financial relationships.
Keerthy Gopalakrishnan, MD1, Himani Mongia, MBBS1, Amit Sohagia, MD2. P6275 - Peritoneal Carcinomatosis as the Initial Sign: An Atypical Presentation of Duodenal Adenocarcinoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.