Udita Gupta, MD1, Prithvi Reddy Akepati, MD1, Pooja Viswanath, DO2, Alan Gabriel. Ortega Macias, MD2, Gulshan Parasher, MD, FACG2 1University of New Mexico Hospital, Albuquerque, NM; 2University of New Mexico, Albuquerque, NM Introduction: Primary gastric squamous cell carcinoma (PGSCC) is an exceptionally rare malignancy. Since its first description in 1895, fewer than 100 cases have been reported, comprising 0.04–0.07% of all gastric cancers. Its pathogenesis remains unclear, and treatment strategies are not standardized. The disease carries a poor prognosis, with a median survival of 7 months.
Case Description/
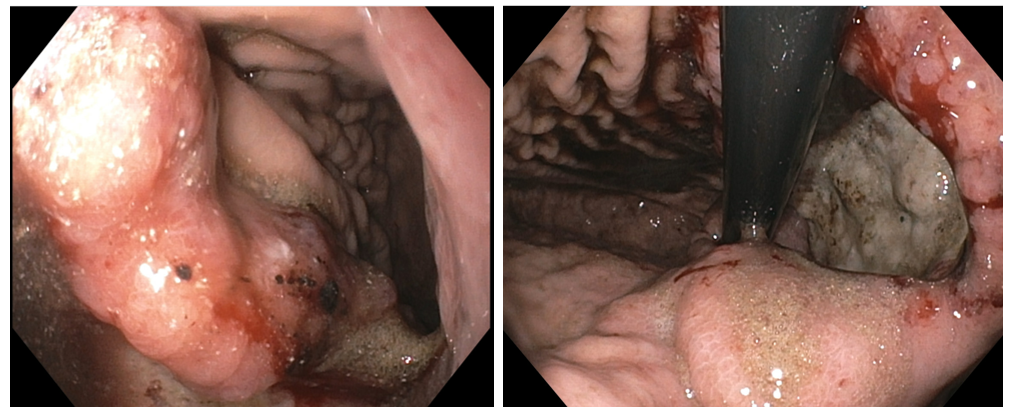
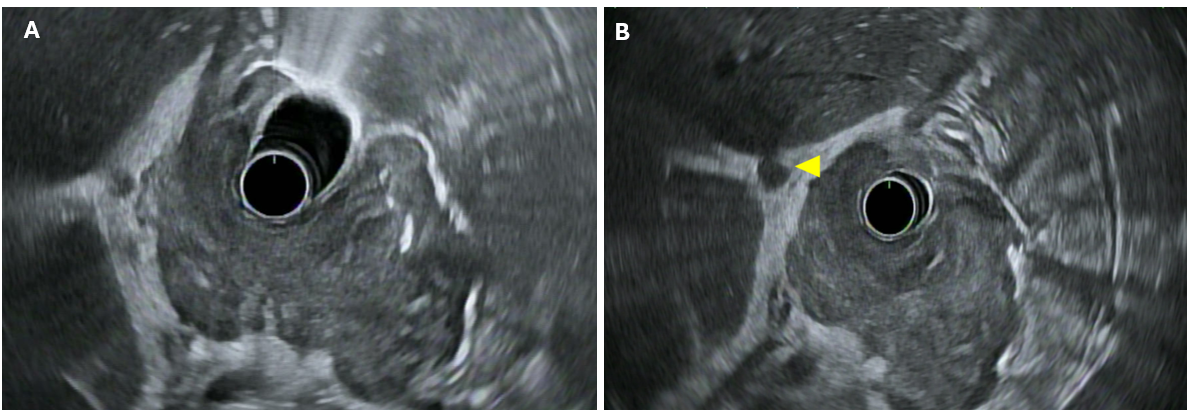
Methods: A 71-year-old Navajo male with a 50+ pack-year smoking history presented with 8 weeks of abdominal pain and intermittent hematemesis. He reported a 1-year history of reduced appetite and unintentional weight loss of 30 lbs. Exam was unremarkable. Labs revealed microcytic iron-deficiency anemia (hemoglobin 9.3 g/dL, MCV 77 fL). He noted that a prior CT scan performed at an outside hospital 6 months earlier had shown gastric ulceration suspicious for malignancy, but he was lost to follow-up. EGD revealed a 4 cm fungating, centrally ulcerated mass involving the cardia, fundus, and proximal body. (Fig 1) Biopsy confirmed invasive squamous cell carcinoma. Immunohistochemistry showed strong p63 positivity and patchy CK7 expression, consistent with squamous differentiation. HER2 was negative, and H. pylori was not detected. EUS demonstrated a hypoechoic mass along the lesser curvature with sonographic evidence of serosal invasion and peri-gastric lymphadenopathy. (Fig 2) Per endosonographic criteria, the tumor was staged at least T3N1Mx (T4 could not be excluded). No distant metastases were identified on CT scan. Despite good performance status (ECOG 0), the patient had an aggressive disease course and died at home within 8 weeks of diagnosis before treatment could be initiated. Discussion: This case exemplifies the typical clinical presentation of rare PGSCC. Although epidemiologic data are scarce, PGSCC predominantly affects men over 60 years of age and is more prevalent among African Americans. In addition, patients tend to be in advanced stages of disease compared to gastric adenocarcinoma. Due to its rarity, no standardized treatment guidelines exist. Surgical resection (total gastrectomy with D2 lymphadenectomy) is the reported treatment. Use of adjuvant chemotherapy and radiotherapy varies widely in literature. Given PGSCC’s poor prognosis, early endoscopy with tissue sampling, multidisciplinary care, and proactive patient engagement are critical to improving outcomes. In underserved demographics such as the one our patient belongs to, limited access to care and delayed follow-ups exacerbate diagnostic delays.
Figure: Fig 1: Esophagogastroduodenoscopy showing fungating and ulcerated gastric mass involving gastric cardia, fundus and proximal body
Figure: Fig 2: Endoscopic ultrasound showing A) bulky tumor involving serosal layer of stomach (layer 5). B) perigastric lymph node
Disclosures: Udita Gupta indicated no relevant financial relationships. Prithvi Reddy Akepati indicated no relevant financial relationships. Pooja Viswanath indicated no relevant financial relationships. Alan Ortega Macias indicated no relevant financial relationships. Gulshan Parasher indicated no relevant financial relationships.
Udita Gupta, MD1, Prithvi Reddy Akepati, MD1, Pooja Viswanath, DO2, Alan Gabriel. Ortega Macias, MD2, Gulshan Parasher, MD, FACG2. P6336 - Primary Gastric Squamous Cell Carcinoma: A Rare Case Highlighting the Need for an Early Diagnosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.