University of Texas Health Science Center at San Antonio San Antonio, TX
Ruayda Bouls, MD1, Anudeeksha Satheeshkumar, MD2, Erin Kaser, DO3, Ally Wong, BS3, Jonathan Yang, BS3, Andrew R. Gonzalez, MD3 1University of Texas Health San Antonio, San Antonio, TX; 2University of Texas Health Science Center at San Antonio, San Antonio, TX; 3University of Texas Health Sciences Center at San Antonio, San Antonio, TX Introduction: Hepatic brucelloma is a very rare complication of brucellosis. We present a case of a patient without any signs of liver injury or decompensation with hepatic brucelloma as his primary manifestation of brucellosis.
Case Description/
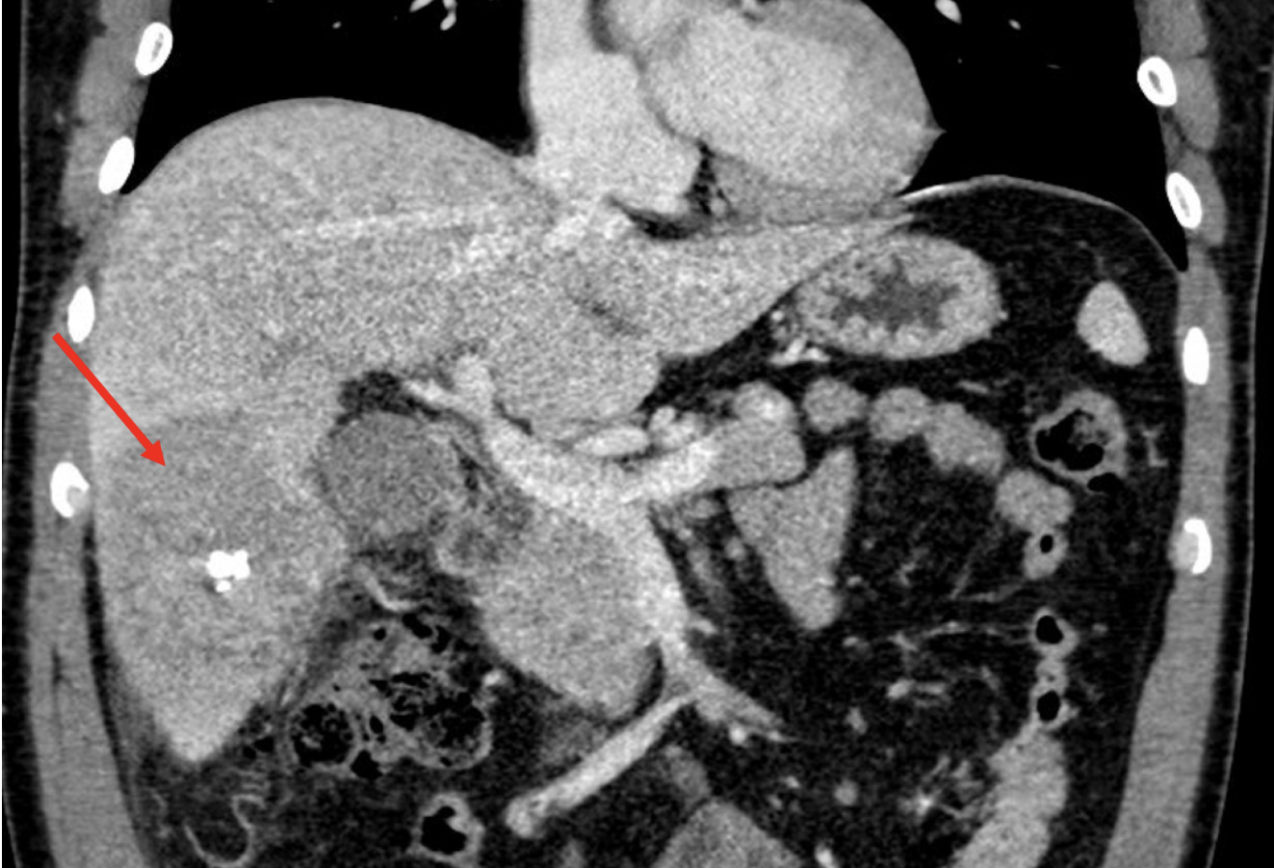
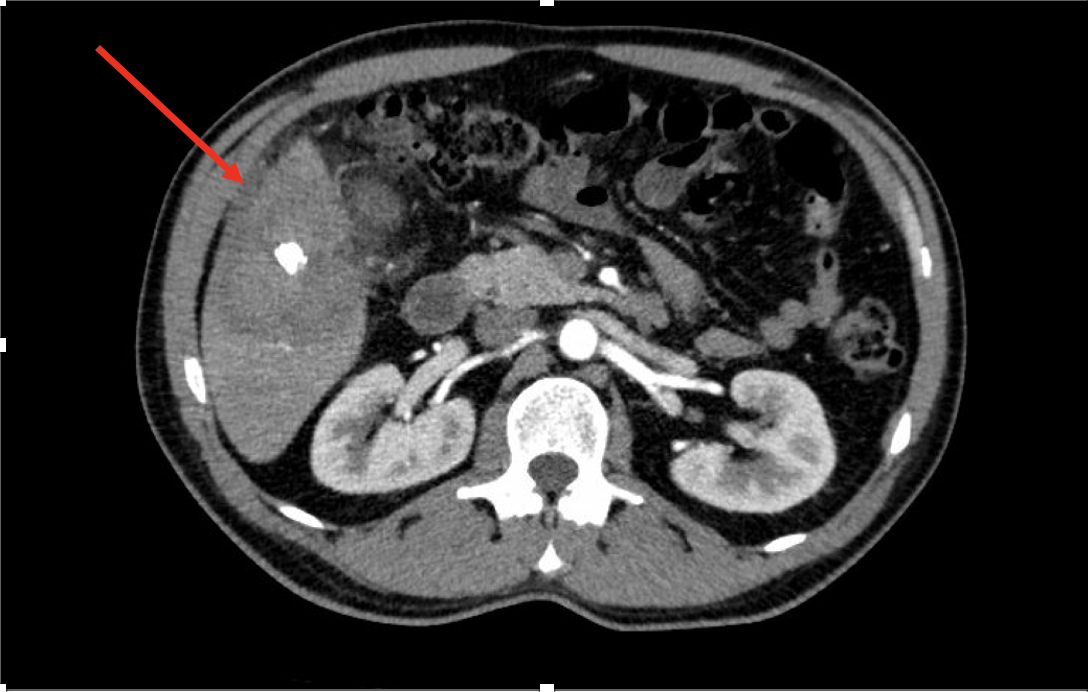
Methods: A 44-year-old male from Mexico with past medical history of hypertension, hyperlipidemia, and uncomplicated diverticulosis presents with five days of sharp right upper quadrant (RUQ) pain. Patient was afebrile and hemodynamically stable on admission. Initial labs showed mild leukocytosis at 10.5 K/mcl. AST and ALT were 17 U/L and 21 U/L, respectively. Total bilirubin was 0.5 mg/dL and alkaline phosphatase was 84 U/L. Initial RUQ ultrasound showed a large 10 cm right-lobe hepatic mass with internal hyperechoic focus. Four-phase liver CT scan showed an indeterminate hypoenhancing lesion measuring 7.1 cm within hepatic segments 5/6 without arterial enhancement with central calcification and a small hypoenhancing peripheral enhancing portion in the exophytic location, concerning for malignancy versus infection. Ceftriaxone and metronidazole were started for empiric treatment of liver abscess. Initial infectious workup resulted negative. Tumor markers CA 19-9, AFP, and CEA were negative. A colonoscopy was negative for any findings. Notably, Brucella antibody titer resulted positive at 1:80 (normal < 1:20). Biopsy of the hepatic lesion revealed extensive granulomatous inflammation with abundant reactive plasma cells. Karius testing was completed and was positive for Brucella melitensis. Patient was transitioned to gentamicin, doxycycline, and rifampin. Discussion: Brucellosis is caused by the gram-negative bacteria, Brucella spp. Infection occurs after ingestion of contaminated food or through direct contact with infected animals via ruptured skin/mucosa. Brucellosis has many non-specific clinical manifestations, including fever, cough, arthralgia, abdominal pain, and fatigue. The bacteria has an affinity for reticuloendothelial cells, 90% of which are located in the liver. A brucelloma is an area of necrotic granulomatous tissue caused by the presence of the bacteria within macrophages. In this patient, despite very minimal clinical manifestations of infection and absence of any liver injury markers, the presence of RUQ pain and liver mass on imaging prompted an extensive evaluation, leading to the discovery of hepatic brucelloma. This case highlights the importance of thoroughly evaluating any hepatic mass, even without signs of liver injury or decompensation.
Figure: Coronal CT abdomen/pelvis image showing large hypoenhancing hepatic mass with central calcification in hepatic segments 5/6
Disclosures: Ruayda Bouls indicated no relevant financial relationships. Anudeeksha Satheeshkumar indicated no relevant financial relationships. Erin Kaser indicated no relevant financial relationships. Ally Wong indicated no relevant financial relationships. Jonathan Yang indicated no relevant financial relationships. Andrew Gonzalez: Eli Lilly – Stock-publicly held company(excluding mutual/index funds). Pfizer – Stock-privately held company.
Ruayda Bouls, MD1, Anudeeksha Satheeshkumar, MD2, Erin Kaser, DO3, Ally Wong, BS3, Jonathan Yang, BS3, Andrew R. Gonzalez, MD3. P6085 - Oh Ma! Brucelloma!, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")