Xavier Zonna, DO1, Lan Nguyen, DO1, Conor Banta, MD2 1University at Buffalo, Buffalo, NY; 2Geisinger Commonwealth School of Medicine, Providence, RI Introduction: The urachus is an embryological structure that forms a drainage site for the fetal bladder by connecting with the umbilicus from the bladder. When the fetus is delivered, the urachus normally closes and becomes a ligamentous structure. Urachal carcinoma is a rare malignant tumor that can arise from failure of closure during development. This case illustrates liver metastases, peritoneal carcinomatosis, and malignant ascites as sequelae of this disease.
Case Description/
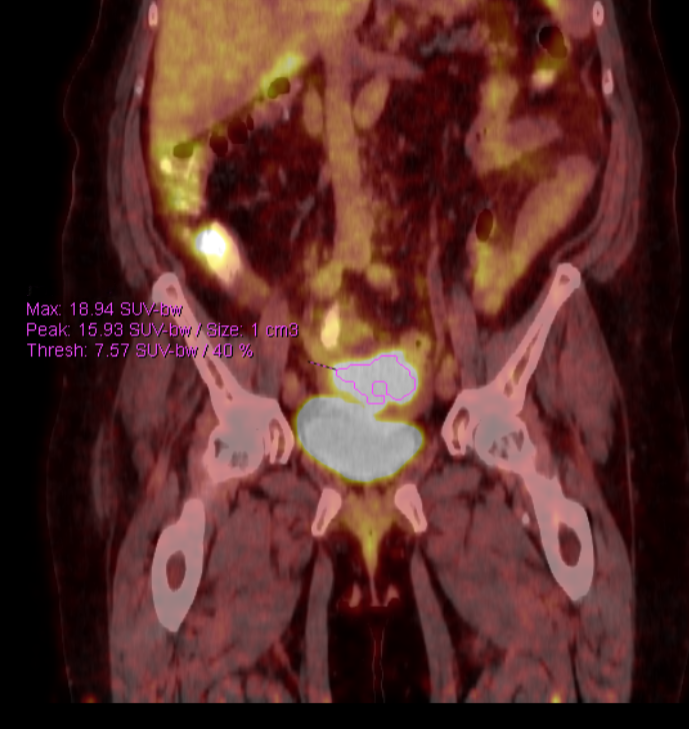
Methods: A 68-year-old female presented with nausea, vomiting, and umbilical swelling. As initial CT AP revealed a possible ovarian mass, PET imaging was obtained, revealing a primary central mass superior to the bladder 7.9 x 6.4 cm with preserved separation and hepatic metastasis (Figure 1). Biopsy revealed poorly differentiated carcinoma with urothelial features. Cystoscopy was negative for any bladder mass and tumor markers confirmed urachal carcinoma. Several months later, the patient presented to the hospital with several weeks of progressive dyspnea and abdominal distension. The patient's abdomen was distended and non-tender on palpation, in addition to bibasilar rales being noted on lung auscultation. Repeat CT revealed 8.6 x 6.5 cm mass, hepatic metastases, numerous peritoneal implants, and large volume ascites (Figure 2). After undergoing CT-guided thoracentesis and paracentesis with significant improvement, the patient was discharged in stable condition. Discussion: Urachal Carcinoma is an aggressive malignancy that is difficult to treat due to its rarity and lack of substantial evidence behind therapies [1]. Mortality is high, with studies documenting a 5-year survival rate of 51% [1]. Patients commonly present with hematuria due to inferior invasion, making this patient’s original presentation atypical [1]. Patients often present with metastatic disease at initial diagnosis and seeding of the liver and peritoneum may occur. Treatment includes local surgical resection and systemic chemotherapy for metastatic disease. However, specific surgical techniques and chemotherapy regimens are not well established. Recurrence rates are also high and are estimated up to 35% [1]. Providers should be aware of the possibility of liver metastases and ascites secondary to urachal carcinoma.
References:
Suartz CV, Martinez LM, Silvestre MHL, et al., Urachal Carcinomas: A Comprehensive Systematic Review and Meta-analysis. Int Braz J Urol. 2025 May-Jun;51(3):e20240665. doi: 10.1590/S1677-5538.IBJU.2024.0665.
Figure: Figure 1: Initial PET scan with pelvic mass superior to bladder
Figure: Figure 2: CT from admission demonstrating urachal carcinoma superior to bladder in addition to malignant ascites
Disclosures: Xavier Zonna indicated no relevant financial relationships. Lan Nguyen indicated no relevant financial relationships. Conor Banta indicated no relevant financial relationships.
Xavier Zonna, DO1, Lan Nguyen, DO1, Conor Banta, MD2. P6027 - Urachal Carcinoma as an Etiology of Liver Metastases, Peritoneal Carcinomatosis, and Ascites, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.