Robert Wood Johnson Medical School, Rutgers University New Brunswick, NJ
Ankoor Patel, MD, George Abdelsayed, MD Robert Wood Johnson Medical School, Rutgers University, New Brunswick, NJ Introduction: Portal hypertension polyposis (PHP) is a rare complication, occurring in approximately 2.5% of patients with portal hypertension. Iron deficiency anemia (IDA) in patients with cirrhosis are typically due to varices, portal hypertensive gastropathy, or gastric antral vascular ectasia. However, we report a rare case of IDA in a patient with PHP with bleeding.
Case Description/
Methods: A 74-year-old male with a history of decompensated cirrhosis 2/2, coronary artery disease (CAD), and gout presents to hepatology clinic for dyspnea on exertion, generalized weakness, and fatigue. He reported no changes to his medications and denied toxic habits, including alcohol use, smoking, or illicit drug use.
Initial laboratory work revealed anemia (hemoglobin 8.5 g/dL), thrombocytopenia (81,000/µL), mild elevations in LFT’s and total bilirubin. Nutritional studies indicated normal B12 and folate levels, while iron studies confirmed IDA. Six months prior, hemoglobin was recorded at 10.2 g/dL with normal iron studies. The patient began oral iron supplementation but demonstrated minimal improvement in iron parameters.
He was up-to-date with colonoscopy for colorectal cancer (CRC) screening, with the last procedure three years earlier revealing two small polyps. His esophagogastroduodenoscopy (EGD) for esophageal variceal (EV) screening showed grade I EV, mild portal hypertensive gastropathy, and gastric polyps. Recent hepatocellular carcinoma (HCC) surveillance with MRI yielded no evidence of malignancy and normal alpha-fetoprotein levels.
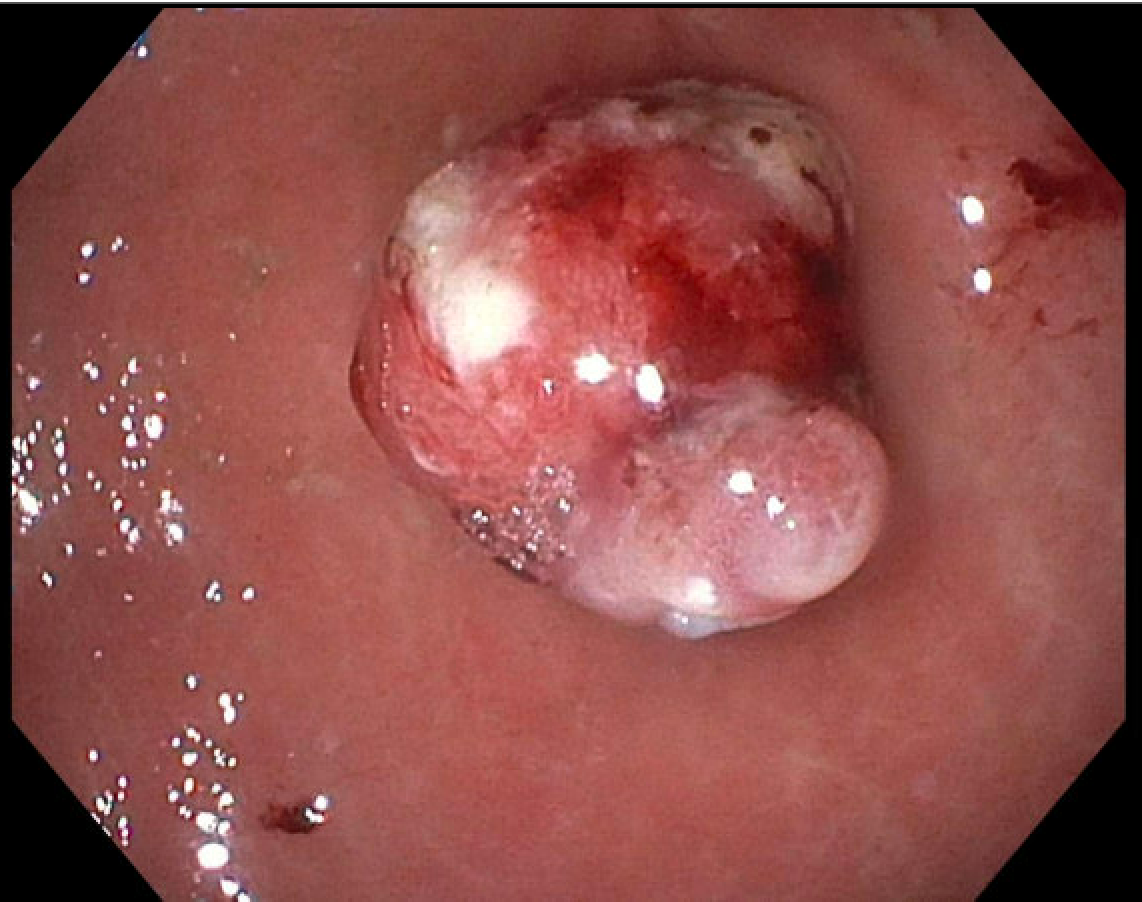
An EGD was performed as he was due for screening purposes to evaluate for esophageal varices. EGD showed grade I esophageal varices, mild portal hypertensive gastropathy, four gastric polyps were identified and biopsied, confirming hyperplastic changes. One polyp exhibited signs of recent bleeding, evidenced by an overlying blood clot and ulceration upon lavage and removal of the blood clot. The polyp was excised using hot snare polypectomy, and a clip was applied to mitigate post-polypectomy bleeding. Histopathological examination confirmed the diagnosis of a hyperplastic polyp with focal ulceration measuring up to 1.5 cm. Gastric biopsies indicated mildly active gastritis without H. pylori infection.
Following EGD, patient has experienced a gradual improvement in hemoglobin levels. Discussion: When evaluating patients for IDA or who are due for EV screening, clinicians should also consider portal hypertension polyposis as a potential source of complications in this population.
Figure: Image of portal hypertensive associated polyp with stigmata of recent bleeding and area of ulceration.
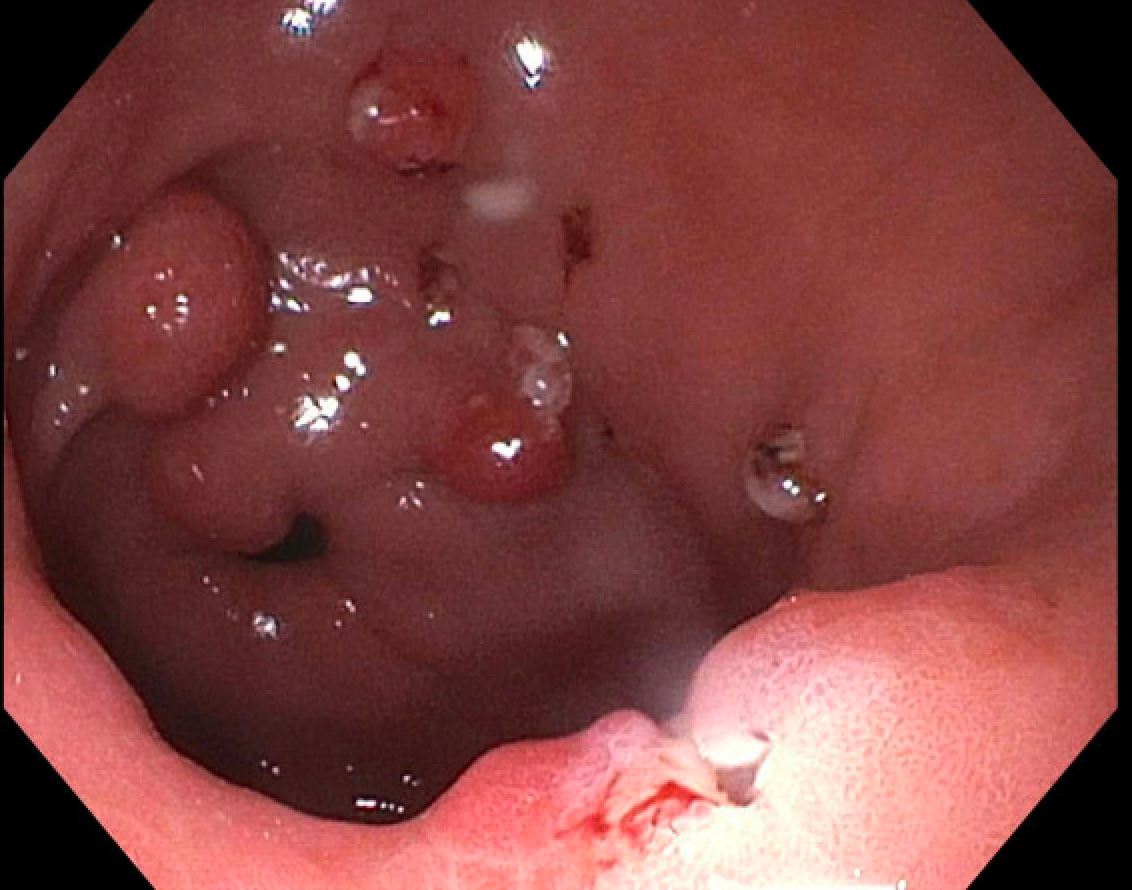
Figure: Image of multiple portal hypertensive associated polyp and following polypectomy of bleeding antral polyp.
Disclosures: Ankoor Patel indicated no relevant financial relationships. George Abdelsayed indicated no relevant financial relationships.
Ankoor Patel, MD, George Abdelsayed, MD. P6001 - A Unique Cause of IDA in a Patient With Decompensated Cirrhosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.