Mauricio Jones, DO1, Maxwell A. Jones, MD2, Tyler Cobbs, DO3 1Oklahoma State University, Tulsa, OK; 2University of Arkansas for Medical Sciences, Little Rock, AR; 3oklahoma state university, Phoenix, AZ Introduction: Chronic liver disease is commonly attributed to intrinsic hepatic pathology, but less frequently recognized is hepatic congestion due to cardiac causes. Constrictive pericarditis, although rare, may mimic features of cirrhosis and lead to diagnostic confusion. We present a case of chronic liver disease initially attributed to cirrhosis, ultimately diagnosed as congestive hepatopathy secondary to constrictive pericarditis.
Case Description/
Methods: A 74-year-old woman with a history of atrial fibrillation and congestive heart failure was referred for evaluation of chronic liver disease. She denied prior liver disease but had a history of hepatic steatosis and progressive ascites requiring paracentesis. Imaging revealed cirrhotic morphology on ultrasound, yet prior CT abdomen showed normal liver morphology with prominent IVC and hepatic veins, suggestive of congestive hepatopathy. Laboratory evaluation showed normal liver enzymes, mildly elevated bilirubin (1.6 mg/dL), and preserved synthetic function. Ascitic fluid analysis revealed high-protein ascites. Portal pressure readings demonstrated elevated FHVP and WHVP with normal HVPG, consistent with post-hepatic portal hypertension. Liver biopsy revealed early bridging fibrosis and sinusoidal dilation, without cirrhosis or steatosis, suggestive of cardiac hepatopathy. Cardiac catheterization showed equalization of diastolic pressures and a dip-and-plateau pattern, diagnostic of constrictive pericarditis. The patient underwent successful pericardiectomy with subsequent clinical improvement. Discussion: This case highlights the diagnostic challenge of differentiating cirrhosis from cardiac-induced liver disease. Constrictive pericarditis can cause hepatic congestion, mimicking cirrhosis clinically and radiographically. High-protein ascites, normal HVPG, and sinusoidal dilation on biopsy should raise suspicion for congestive hepatopathy. Early identification of cardiac causes can redirect management and prevent unnecessary interventions. Pericardiectomy can be curative, emphasizing the importance of a multidisciplinary approach in evaluating unexplained chronic liver disease.
Generative AI (ChatGPT, OpenAI) was utilized to assist with drafting and refining the language of this abstract. All clinical content was reviewed and verified by the authors.
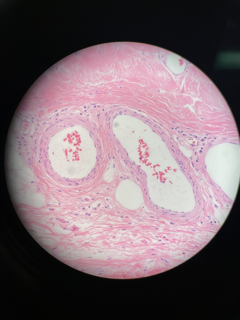
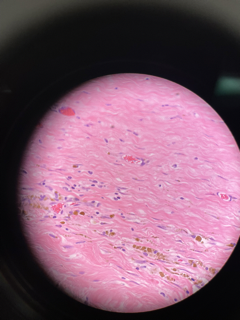
Figure: Pericardial Biopsy
Figure: Pericardial Biopsy
Disclosures: Mauricio Jones indicated no relevant financial relationships. Maxwell Jones indicated no relevant financial relationships. Tyler Cobbs indicated no relevant financial relationships.
Mauricio Jones, DO1, Maxwell A. Jones, MD2, Tyler Cobbs, DO3. P5998 - High Protein Ascites: Hepatology vs Cardiology, Is This from Liver?, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.