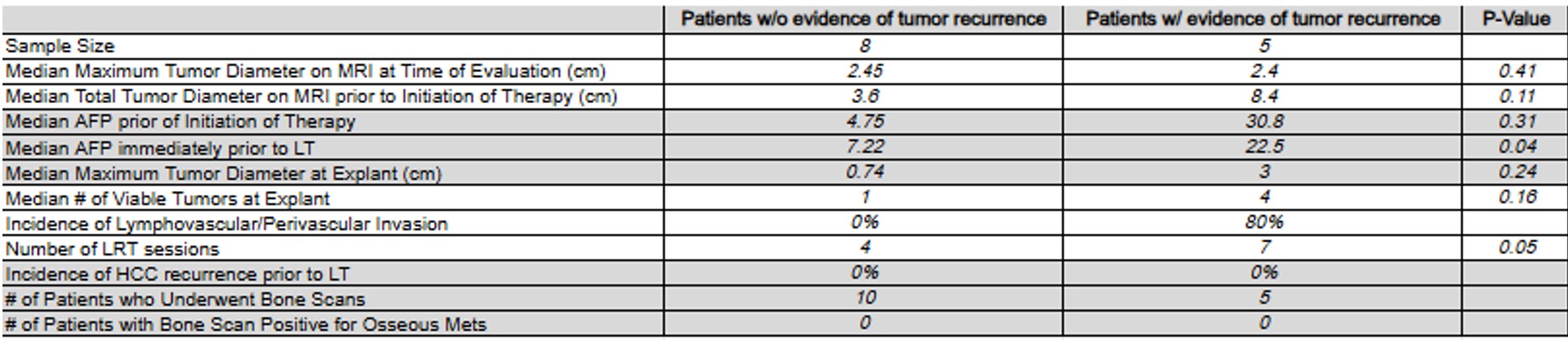
Khadyoth Nanneboyina, MD1, Ali Khurram, MD1, Ashwini Mehta, DO2, Judith Pozzerle, RN1, Parvez Mantry, MD, CPE1 1Methodist Dallas Medical Center, Dallas, TX; 2Dallas Methodist, Dallas, TX Introduction: Liver transplantation (LT) is the gold standard treatment for unresectable Hepatocellular Carcinoma (HCC). As patients undergo transplant evaluation, bridging therapies are used to treat HCC lesions such as locoregional therapies (LRT). There is a strong rationality to use systemic therapy as a bridging therapy alongside LRT. However, there remain knowledge gaps on the impact of these systemic therapies on tumor recurrence. Methods: This study was a single-center retrospective outcome analysis of all patients diagnosed with HCC recurrence in patients who underwent LT after receiving systemic therapy along with locoregional therapy (LRT) between June 2018 and March 2024 (n = 15). The primary endpoint was post-LT tumor recurrence and overall survival. Evidence of tumor recurrence was based on imaging evidence and positive molecular tumor marker such as Signatera or elevation in traditional tumor markers such as Alpha-fetoprotein (AFP). Patients who had evidence of recurrence were compared to patients who did not have recurrence. Systemic therapies included Nivolumab + Ipilimumab, Atezolizumab + Bevacizumab, Sorafenib, Lenvatinib, Ramuricumab, and Cabozantinib. The T-test was used. Results: 5 patients had tumor recurrence, and 8 patients did not. 2 patients were excluded from analysis as 1 had intraoperative cardiac arrest and another patient died of systemic inflammatory response syndrome possibly secondary to COVID pneumonia 12 days postop. Median Total Tumor Diameter prior initiation of systemic therapy was 3.6 in recurrence group and 8.4 in nonrecurrence group, however this did not achieve statistical significance (p = 0.11). Median alpha-fetoprotein immediately prior to transplant was 7.22 in recurrence group and 22.5 in nonrecurrence group (p = 0.04). The number of received LRT therapies was 7 in recurrence group and 4 in nonrecurrence group (p = 0.05). Discussion: We observed that systemic therapy prior to LT had higher tumor recurrence. Even though initial median total tumor diameters were similar in the start, the recurrence group had a higher AFP which appears to be statistically significant. Certainly, the group with recurrence had received more locoregional therapies indicating a worse tumor biology. These factors will need to be considered for high-risk patients prior to transplantation with perhaps better adjudication of wait time prior to transplant to better assess tumor biology better. Certainly, more data is needed and should continue to accrue at transplant centers.
Figure: Table 1. Tumor characteristics of patients with and without recurrence when receiving combination therapy.