University of Iowa Hospitals & Clinics Iowa City, IA
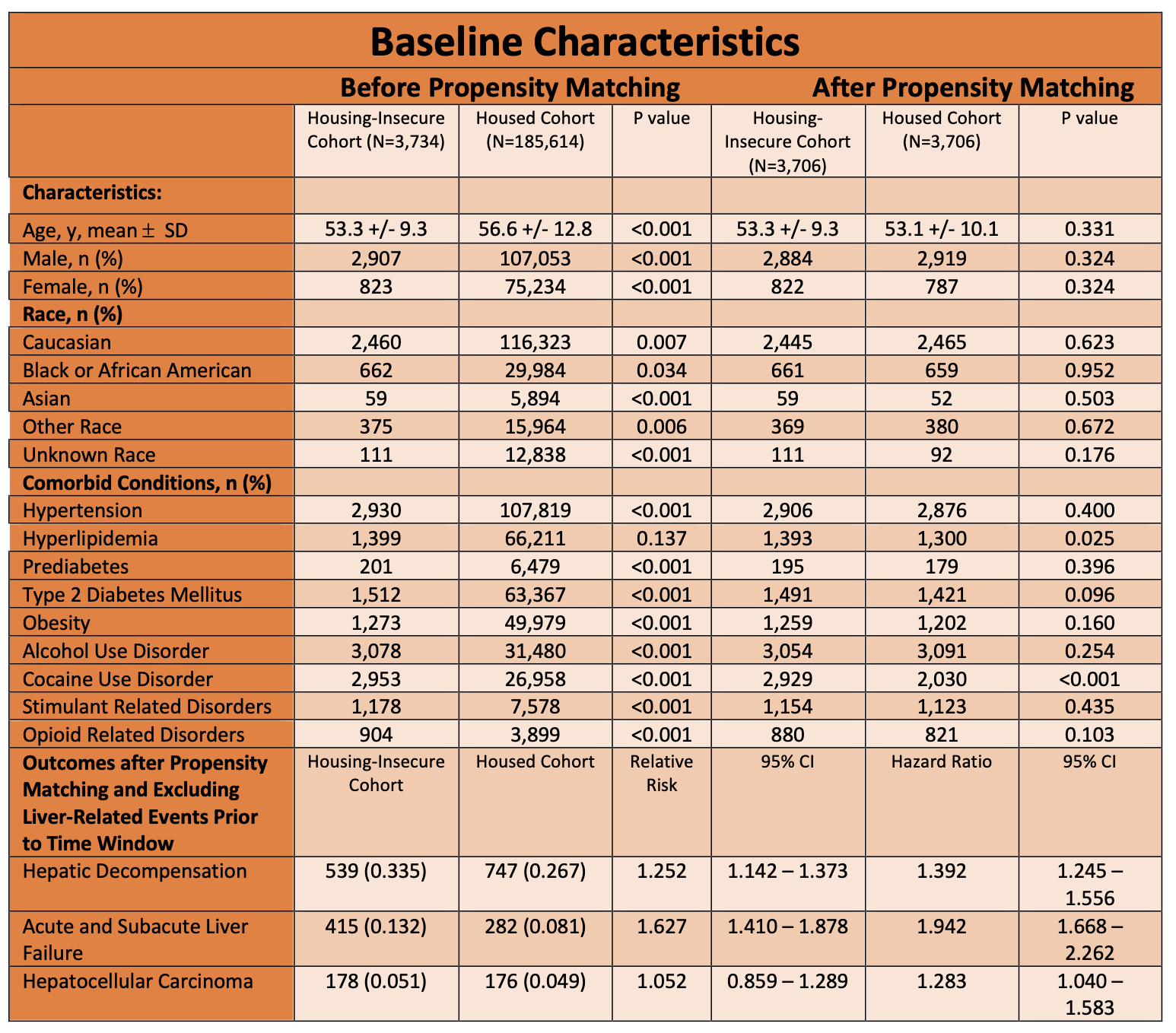
Alp S. Kahveci, MD1, Abdullah Sohail, MD1, Antonio Sanchez, MD2 1University of Iowa Hospitals & Clinics, Iowa City, IA; 2University of Iowa Hospitals and Clinics, Iowa City, IA Introduction: In the United States, 2.3 to 3.5 million people experience homelessness annually. In this population, the prevalence of mental health disorders and chronic medical conditions, as well as morbidity and mortality, are increased relative to the general population. The influence of homelessness and/or housing instability on decompensated cirrhosis is still not fully appreciated. We sought to investigate the real-world influence of these risk factors on the subsequent development of hepatic decompensation. Methods: This study was designed utilizing the TriNetX US Collaborative Network, which encompasses a total of 13,107,240 patients aged ≥ 18 years. Patients were categorized into two cohorts via ICD-10 codes: housed patients with cirrhosis and patients with cirrhosis who experienced homelessness or housing instability within a year after diagnosis. Propensity score matching was used to balance cohorts by age, sex, race, and co-morbidities (HTN, HLD, T2DM or prediabetes, obesity, AUD, and injection drug use (cocaine, opioids, amphetamines)). Primary outcomes were the development of hepatic decompensation (ascites, variceal bleed, or hepatic encephalopathy) over a lifetime. Secondary outcomes included the development of acute and subacute liver failure and hepatocellular carcinoma. Patients with a pre-existing history of a primary or secondary outcome were excluded. Results: Following propensity score matching, 3,706 patients were included in each cohort. Among those with homelessness or housing instability, 33.45% experienced hepatic decompensation compared to 26.72% in the housed cohort (relative risk [RR] 1.252; 95% CI, 1.142–1.373). Kaplan–Meier analysis demonstrated a projected lifetime survival probability of 34.24% for the housing-insecure cohort and 52.44% for the housed cohort (hazard ratio [HR] 1.392; 95% CI, 1.245–1.556).
For secondary outcomes, housing-insecure individuals exhibited an increased risk of acute and subacute liver failure (RR 1.627; 95% CI, 1.410–1.878) but no significant difference in HCC incidence (RR 1.052; 95% CI, 0.859–1.289). Discussion: Experiencing homelessness and/or housing instability shortly after diagnosis of cirrhosis is an independent risk factor for the lifetime occurrence of hepatic decompensation events and acute and subacute liver failure. Targeted health policy initiatives aimed at enhancing access to preventative care and chronic disease management for this vulnerable population may help reduce liver-related morbidity and mortality.
Figure: Table 1: Baseline Characteristics and Liver-Related Events
Disclosures: Alp Kahveci indicated no relevant financial relationships. Abdullah Sohail indicated no relevant financial relationships. Antonio Sanchez indicated no relevant financial relationships.
Alp S. Kahveci, MD1, Abdullah Sohail, MD1, Antonio Sanchez, MD2. P3661 - Housing Insecurity Is an Independent Risk Factor for Decompensated Cirrhosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.