KiBeom Kwon, MD1, Grace E. Kim, MD2, Dennis Chen, MD2 1Virginia Mason Franciscan Health, Seattle, WA; 2University of Chicago Medicine, Chicago, IL Introduction: Biliary anastomotic strictures are a well-known complication following liver transplantation. We present a unique case of a post-liver transplant anastomotic stricture that was initially not traversable during ERCP, due to a nearly obstructing stone which was only identified on cholangioscopy.
Case Description/
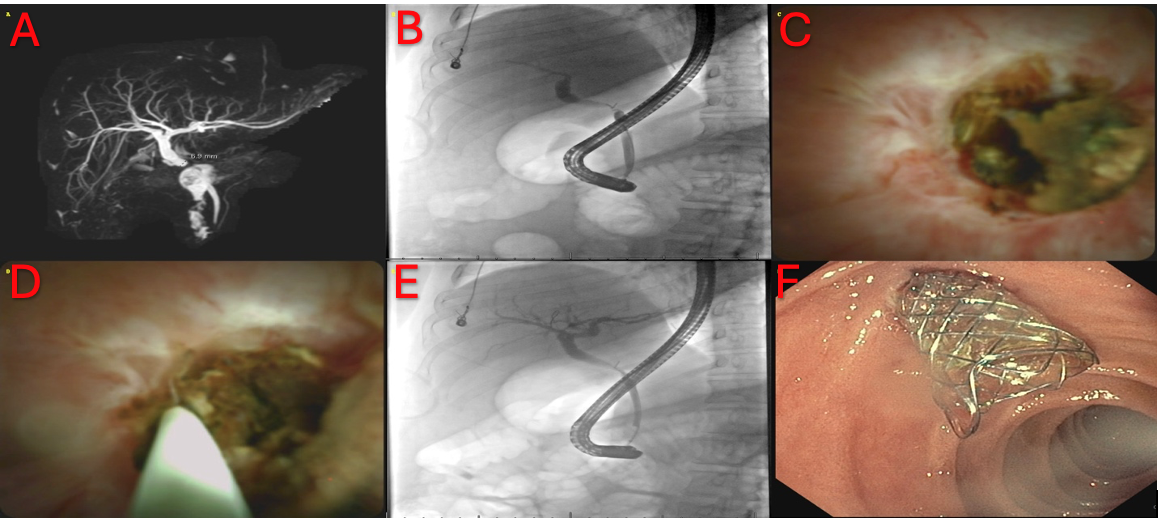
Methods: A 29-year-old male with alcohol-associated cirrhosis who underwent orthotopic liver transplant 9 months earlier presented with elevated liver enzymes, with alkaline phosphatase (ALP) of 227 U/L (30-120 U/L), aspartate aminotransferase (AST) of 75 U/L (8-37 U/L), alanine transaminase (ALT) of 193 U/L (0-50 U/L), and total bilirubin of 0.2 mg/dL (0.1-1.0 mg/dL). MRCP revealed a stricture at the level of anastomosis with upstream biliary dilation to 7 mm (Figure 1A). ERCP was performed with a severe stricture identified on cholangiogram. Attempts to traverse the stricture with multiple devices were initially unsuccessful (Figure 1B). Cholangioscopy was performed for direct visualization. This revealed an impacted stone at the anastomotic stricture, nearly completely obstructing the biliary lumen (Figure 1C). A guidewire was advanced through the cholangioscope past the stone under direct visualization into the donor biliary ducts (Figure 1D). This allowed for stone extraction via balloon sweeps. The final cholangiogram showed a severe anastomotic stricture with dilated upstream ducts (Figure 1E). The stricture was treated with balloon dilation to 4 mm and placement of a 10 mm x 8 cm fully covered metal biliary stent (Figure 1F). The patient’s liver enzymes normalized within 1 week of the procedure. Discussion: Biliary anastomotic strictures are effectively managed with ERCP. In this case, standard techniques could not traverse an apparent severe stricture. Adjunctive cholangioscopy revealed a near-complete obstructing stone impacted at the anastomotic stricture, which had not previously been identified on imaging or cholangiogram. Cholangioscopy enabled successful wire passage into the donor bile ducts and subsequent stone extraction and stricture management. This case highlights the value of cholangioscopy in technically challenging strictures. When conventional ERCP fails, cholangioscopy is a valuable tool for diagnosis and management.
Figure: 1A: MRCP demonstrating biliary anastomotic stricture with proximally dilated duct. 1B: Cholangiogram showing a severe stricture at the level of the anastomosis. 1C: Cholangioscopy showing a nearly occluding stone impacted in the anastomotic stricture. 1D: Cholangioscopy-assisted wire passage beyond the stone. 1E: Cholangiogram showing anastomotic stricture and upstream duct dilation. 1F: Transpapillary metal biliary stent placement across the stricture.
Disclosures: KiBeom Kwon indicated no relevant financial relationships. Grace Kim indicated no relevant financial relationships. Dennis Chen indicated no relevant financial relationships.
KiBeom Kwon, MD1, Grace E. Kim, MD2, Dennis Chen, MD2. P3607 - Cholangioscopy-assisted Identification of an Impacted Stone Within a Biliary Anastomotic Stricture, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpeg.jpg "KiBeom Kwon, MD (he/him/his) photo")