Division of Gastroenterology and Hepatology, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA Chapel Hill, NC
Millie D. Long, MD, FACG1, Yasmmyn D. Salinas, PhD, MPH2, Teresa Bufford, PhD2, Julie M. Crawford, MD2, Derek R. Gazis, MS2, Kathleen Hurwitz, ScD2, Ebuwa Igho-Osagie, MBBS, DPH, MBA3, Gui Liu, PhD, MPH4, Jeremy Shao, MD, PhD5, Bruce E. Sands, MD, MS, FACG6 1Division of Gastroenterology and Hepatology, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA, Chapel Hill, NC; 2Target RWE, Durham, NC; 3Merck, Rahway, NJ; 4Merck Sharp & Dohme LLC, Philadelphia, PA; 5Merck & Co, South San Francisco, CA; 6Dr. Henry D. Janowitz Division of Gastroenterology, Icahn School of Medicine at Mount Sinai, New York, NY, USA, New York, NY Introduction: The Treat-to-target approach in ulcerative colitis (UC) emphasizes proactive monitoring and early treatment adjustment to meet primary treatment targets of clinical and endoscopic remission. However, data on real-world application of these strategies remains limited. We evaluated post-treatment monitoring, remission, and treatment patterns during the first year following initiation of advanced therapy (AT) for UC. Methods: We analyzed data from TARGET-IBD, a longitudinal U.S. registry of patients with clinician-diagnosed IBD. TARGET-IBD includes electronic medical records collected before and after enrollment. Adult patients initiating a new AT (anti IL-12/23, anti-integrin, anti-TNF, JAK inhibitors, S1P modulators) between October 2014 and September 2021 were included for follow-up. Objective reassessment was defined as undergoing endoscopy or fecal calprotectin (FC) testing within 12 months. Remission was evaluated at 2–4 and 10–14 months post-initiation (mimicking induction and maintenance windows). Outcomes included endoscopic remission (Mayo endoscopic subscore = 0 or narrative evidence of inactive disease) and corticosteroid-free remission (no systemic corticosteroid use in the 14 days prior to endoscopy), overall and by line of advanced therapy (first-line [1L] AT vs. second-line or later [2L+] AT). Treatment persistence and corticosteroid use were also summarized. Results: Among 686 UC patients, 51% underwent objective reassessment within 12 months; FC testing was rare (17%). At initiation of AT, 61% had extensive/pancolitis, 33% had left-sided colitis, and 6% had proctitis. At 2-4 months, 61 patients (9%) underwent endoscopy: 21% achieved endoscopic remission and 20% corticosteroid-free remission (Figure 1). At 10-14 months, 144 patients (20%) underwent endoscopy: 29% achieved endoscopic remission and 26% corticosteroid-free remission. At this time window, remission proportions were higher for patients on 1L AT compared to 2L+ AT. Among patients with endoscopy at 10-14 months, 67% required at least one corticosteroid prescription after initiating AT. At 10-14 months, 37% had switched or discontinued their initial AT. Discussion: In this national registry cohort of UC patients initiating a new AT, objective monitoring was infrequent, and corticosteroid use was high over the first year. Remission rates were modest, and many patients required treatment changes. These findings underscore real-world gaps in treat-to-target implementation and early care optimization.
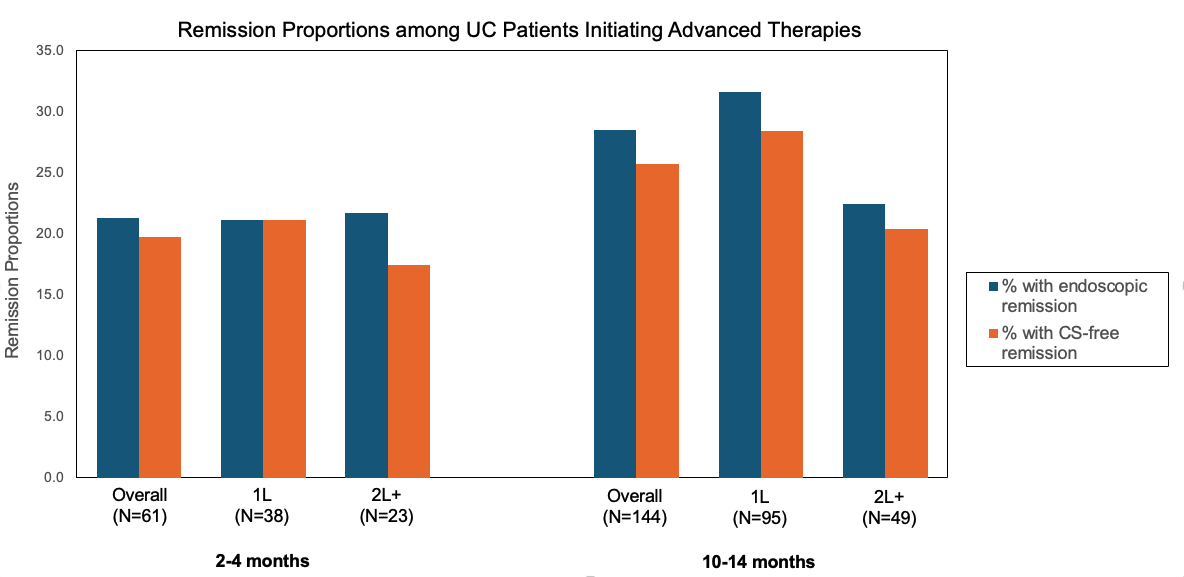
Figure: Figure 1. Remission proportions among ulcerative colitis (UC) patients initiating advanced therapies. Bar graph shows the percentage of patients achieving endoscopic remission (blue) and corticosteroid (CS)-free remission (orange) at 2–4 months and 10–14 months post-treatment initiation, stratified by line of advanced therapy (1L: first-line advanced therapy ; 2L+: second-line or later advanced therapy).