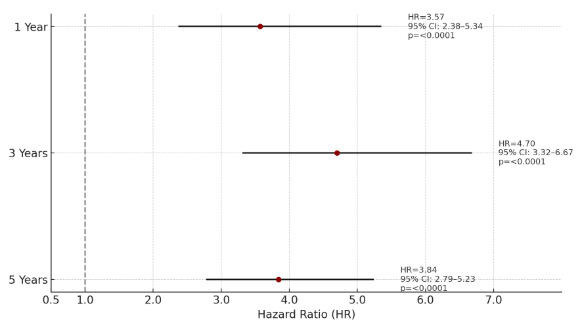
Omar Arman, MD, MPH1, Khaled Rafeh, MD2, Laith M.. Haj-Ahmad, MD3, Kamal Hamad, MD4, Mazen Zamzam, BS5, Jad Bou-Abdallah, MD1 1University at Buffalo, Buffalo, NY; 2School of Medicine, The University of Jordan, Shmeisani, 'Amman, Jordan; 3University of Jordan, Amman, 'Amman, Jordan; 4Jordan University of Science and Technology, Irbid, Irbid, Jordan; 5Oakland University William Beaumont School of Medicine, Royal Oak, MI Introduction: Chronic systemic inflammation in inflammatory bowel disease (IBD) has been implicated in cardiovascular complications, including arrhythmias, yet limited data exist on whether therapy choice modifies this risk. Biologic therapy, through inflammation control, may offer protective cardiac effects. This study evaluates the comparative risk of arrhythmia in IBD patients treated with biologic versus non-biologic therapy over 1, 3, and 5 years. Methods: We analyzed electronic health records from 225,303 adult IBD patients in the TriNetX Research Network. Patients with prior arrhythmias, myocardial infarction, stroke, or heart failure were excluded. Cohorts receiving biologic or non-biologic therapy were propensity score matched for demographics, comorbidities, and disease severity, yielding balanced groups at 1 year (N=16,179), 3 years (N=16,181), and 5 years (N=15,821). Arrhythmia incidence was the primary outcome. We performed Kaplan-Meier survival analysis and calculated risk ratios (RRs), hazard ratios (HRs), and p-values. Results: Non-biologic therapy was associated with consistently higher arrhythmia rates. At 1 year, arrhythmia incidence was 0.66% vs. 0.19% (RR=3.6, 95% CI: 2.38-5.34), with arrhythmia-free survival of 99.12% vs. 99.75% (p< 0.0001, HR=3.57, 95% CI: 2.38-5.34). At 3 years, risk rose further (1.14% vs. 0.23%; RR=4.8, 95% CI: 3.42-6.87), with survival of 98.08% vs. 99.64% (p< 0.0001, HR=4.7, 95% CI: 3.32-6.67). At 5 years, non-biologic therapy had a 1.21% incidence vs. 0.30% (RR=4.1, 95% CI: 2.96-5.59), with survival of 97.50% vs. 99.38% (p< 0.0001, HR=3.84, 95% CI: 2.79-5.23). Mean recurrence scores were also significantly higher in the non-biologic group at 1 year (t = -2.51, p = 0.013) and 5 years (t = -2.94, p = 0.004). Discussion: Biologic therapy is associated with significantly lower arrhythmia risk across all time points in IBD patients. These findings support the role of biologics not only in controlling gut inflammation but also in alleviating cardiovascular risk. Incorporating arrhythmia prevention into therapeutic decisions may improve long-term outcomes. While propensity score matching reduces confounding, prospective studies are needed to confirm these cardioprotective effects.
Figure: Figure. 1 Forest plot showing hazard ratios (HRs) with 95% confidence intervals for arrhythmia risk at 1, 3, and 5 years in IBD patients. Dots indicate HRs; horizontal lines represent CIs. The dashed vertical line at HR=1 marks no difference. Values to the right favor biologic therapy, while values to the left favor non-biologic therapy
Disclosures: Omar Arman indicated no relevant financial relationships. Khaled Rafeh indicated no relevant financial relationships. Laith Haj-Ahmad indicated no relevant financial relationships. Kamal Hamad indicated no relevant financial relationships. Mazen Zamzam indicated no relevant financial relationships. Jad Bou-Abdallah indicated no relevant financial relationships.
Omar Arman, MD, MPH1, Khaled Rafeh, MD2, Laith M.. Haj-Ahmad, MD3, Kamal Hamad, MD4, Mazen Zamzam, BS5, Jad Bou-Abdallah, MD1. P3307 - Comparative Impact of Biologic vs Non-Biologic Therapy on Arrhythmia Risk in Inflammatory Bowel Disease: A 5-Year Propensity-Matched Study, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.