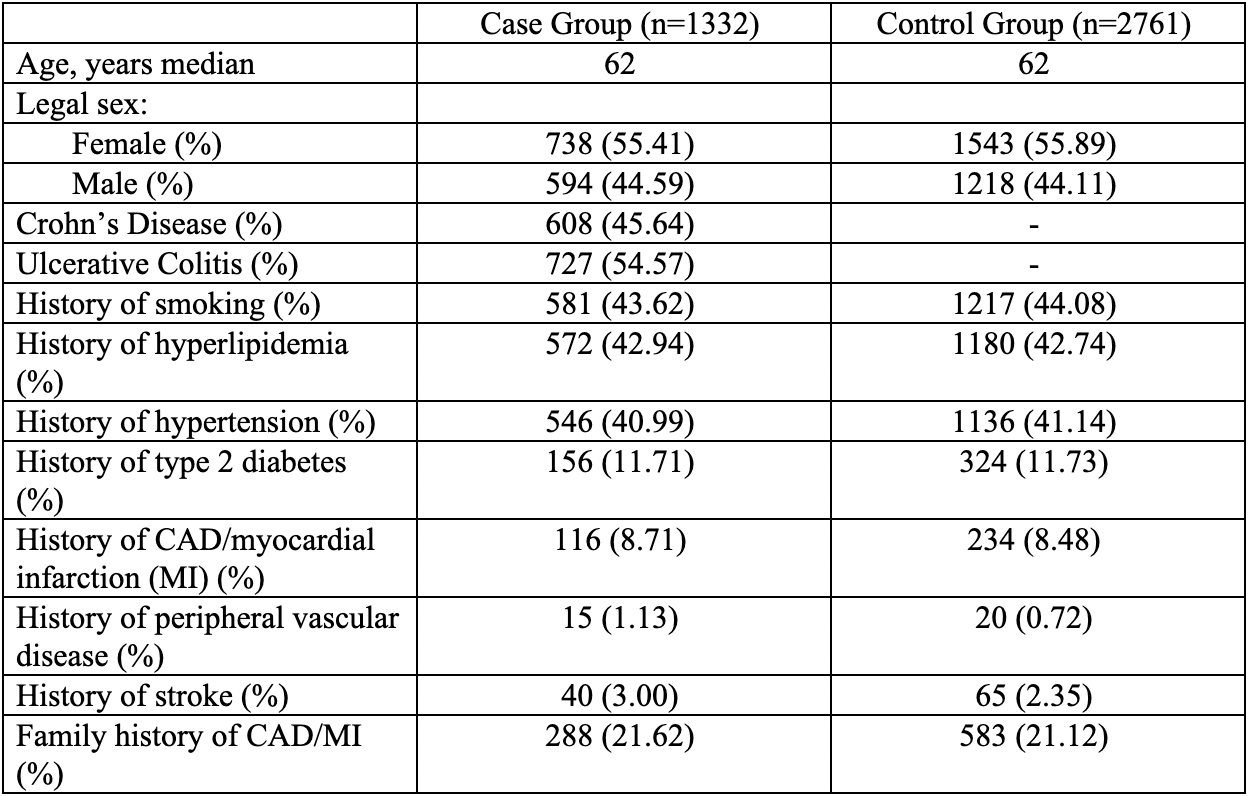
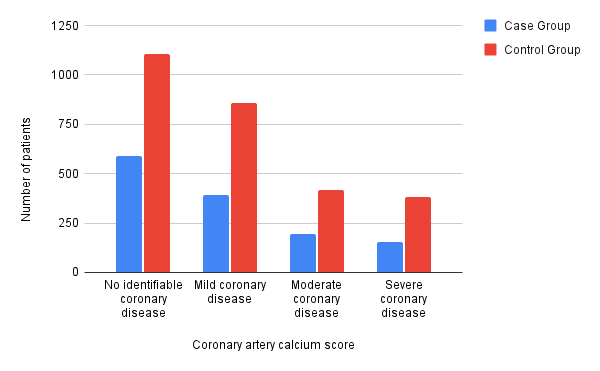
Ashley Robinson, DO1, Sareena Ali, DO2, Yannis Lafazanos, DO2, Lukus Berber, MD2, Saad Hashmi, MD3, Ahmed Khattab, MD, MRCP2, Eli Ehrenpreis, MD, FACG2, Cindy Ndiaye, MPH2 1Advocate Lutheran General, Chicago, IL; 2Advocate Lutheran General, Park Ridge, IL; 3Advocate Condell Medical Center, Lincolnwood, IL Introduction: Prior studies have suggested that patients with inflammatory bowel disease (IBD) have an increased risk of thromboembolic events. However, there is conflicting data regarding risk of atherosclerotic cardiovascular disease (ASCVD) in this patient population, with a prior study at an academic center suggesting higher ASCVD risk for IBD patients assessed by cardiac CT. In this study, we sought to assess ASCVD risk of patients with IBD by comparing coronary artery calcium (CAC) scores in patients with IBD to a matched control group in a community setting. Methods: We performed a retrospective case-control study of adult patients within the Advocate Aurora Health system who had a CAC score CT performed between May 2012 and May 2022. For subjects with multiple studies, the most recent CAC score was collected. The case group included patients with a documented history of IBD. A 2:1 age and sex matched control group was created. Charts were manually reviewed to confirm the presence or absence of IBD based on standard criteria. CAD risk factors, including hypertension, hyperlipidemia, diabetes mellitus, smoking history, and family or personal history of CAD/myocardial infarction, were also collected. CAC scores were divided into four categories: no identifiable coronary disease (CAC score 0), mild coronary disease (1-99), moderate coronary disease (100-399) or severe coronary disease (≥ 400). Categorical data were compared using Chi square, and CAC scores using the Mann Whitney U test. Results: There were 1332 patients in the IBD group and 2761 matched controls (median age 62). Prevalence of CAD risk factors was similar in the case and control populations (Table 1). There was no identifiable CAD in 588 (44.1%) of cases and 1106 (40.1%) of controls, mild disease in 393 (29.5%) versus 857 (31.0%), moderate disease in 196 (14.7%) versus 415 (15.0%), and severe disease in 155 (11.64%) versus 382 (13.84%) respectively (p= 0.0855) (Figure 1). Median CAC scores were 5.0 in the case population and 9.0 in the control group (p= 0.0176). In Crohn’s patients (n= 608), median CAC score was 3.9 versus 6.0 in ulcerative colitis patients (n= 727), (p= 0.6516). Discussion: In our study of a community-based population, IBD patients had lower ASCVD risk compared to controls as assessed by CAC score, suggesting that IBD is not an independent risk factor for CAD.
Figure: Table 1. Baseline characteristics of the study population.
Figure: Figure 1. Level of coronary artery disease in case versus control groups.
Disclosures: Ashley Robinson indicated no relevant financial relationships. Sareena Ali indicated no relevant financial relationships. Yannis Lafazanos indicated no relevant financial relationships. Lukus Berber indicated no relevant financial relationships. Saad Hashmi indicated no relevant financial relationships. Ahmed Khattab indicated no relevant financial relationships. Eli Ehrenpreis: E2Bio Consultants – Intellectual Property/Patents, CEO, Owner/Ownership Interest. E2Bio Life Sciences – CEO, Owner/Ownership Interest. Cindy Ndiaye indicated no relevant financial relationships.
Ashley Robinson, DO1, Sareena Ali, DO2, Yannis Lafazanos, DO2, Lukus Berber, MD2, Saad Hashmi, MD3, Ahmed Khattab, MD, MRCP2, Eli Ehrenpreis, MD, FACG2, Cindy Ndiaye, MPH2. P3186 - Comparison of Coronary Calcium CT Scores in Patients With IBD vs Patients Without IBD, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")