Raya Alashram, MD, Ahmad Abulawi, MD, Stephen Hasak, MD, MPH, Seth Richter, MD, FACG Albany Medical Center, Albany, NY Introduction: Portal hypertension can be classified as cirrhotic or non-cirrhotic. Non-cirrhotic prehepatic portal hypertension is uncommon and often challenging to diagnose typically requiring an extensive workup. It is also a rare complication following pancreatic surgery. We present the case of a 69-year-old female who underwent pancreaticoduodenectomy for pancreatic cancer with portal and splenic vein involvement and subsequently developed complications related to portal hypertension.
Case Description/
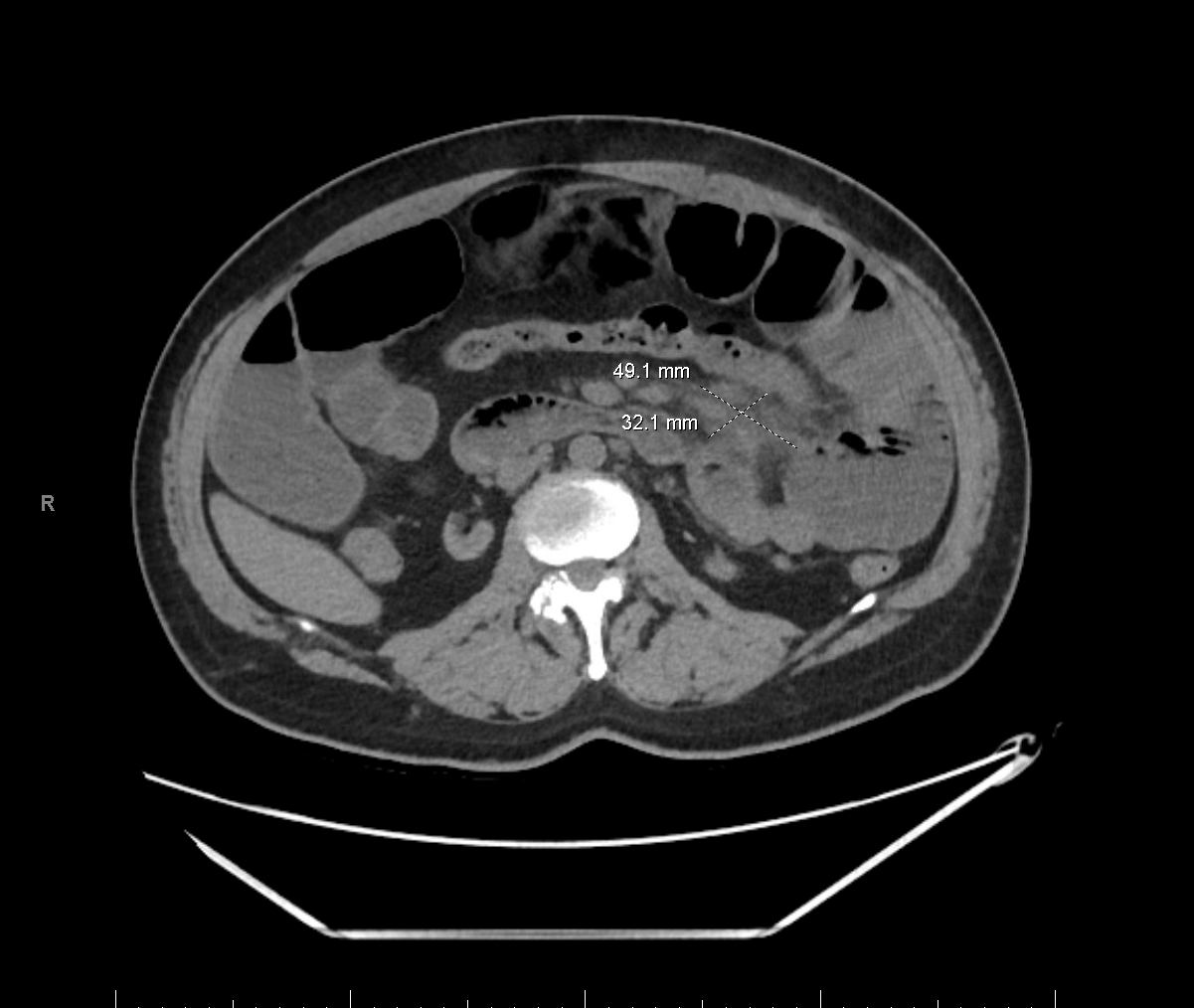
Methods: A 69-year-old female with a history of pancreatic cancer was treated with six cycles of neoadjuvant chemotherapy followed by a pancreaticoduodenectomy (Whipple procedure), which was complicated by portal vein invasion requiring vascular reconstruction. Surveillance imaging showed no evidence of disease recurrence. One year postoperatively, she presented to the emergency department with hematemesis and hematochezia. Laboratory evaluation revealed leukopenia (WBC 2.7 × 10⁹/L), anemia (hemoglobin 44 g/L), and normal platelet count (266 × 10⁹/L). She was resuscitated and underwent emergent esophagogastroduodenoscopy (EGD), which identified bleeding esophageal varices. Hemostasis was achieved via endoscopic band ligation. Further evaluation with contrast-enhanced CT angiography of the abdomen revealed no active bleeding but demonstrated significant stenosis of the portal vein and superior mesenteric vein, consistent with portal hypertension (Figure 1). Interventional radiology performed portal venography followed by venoplasty and portal vein stent placement to relieve the obstruction (Figure 2). A repeat EGD four weeks later showed complete resolution of varices and portal hypertensive gastropathy. Discussion: Portal hypertension following Whipple surgery is an uncommon but recognized complication. Its incidence increases significantly in cases involving vascular resection or reconstruction, with reported rates between 10% and 25%. In contrast, it is rare ( < 5%) following standard Whipple procedures without vascular involvement. This case highlights the importance of considering non-cirrhotic portal hypertension in post-pancreatectomy patients with gastrointestinal bleeding, particularly those with prior portal or mesenteric vein reconstruction. Endoscopic and radiological interventions—including venoplasty and portal stenting—can be effective in relieving portal pressure and preventing recurrent bleeding and other sequela
Figure: Figure 1 CTA abdomen showing significant stenosis of the portal vein and superior mesenteric vein, consistent with portal hypertension.
Figure: Figure 2 Right demonstrates portal vein stenosis Left demonstrates portal vein after stenting
Disclosures: Raya Alashram indicated no relevant financial relationships. Ahmad Abulawi indicated no relevant financial relationships. Stephen Hasak: Castle Biosciences – Speakers Bureau. Conmed – Consultant. Seth Richter indicated no relevant financial relationships.
Raya Alashram, MD, Ahmad Abulawi, MD, Stephen Hasak, MD, MPH, Seth Richter, MD, FACG. P3101 - No Cirrhosis, No Problem? A Hidden Case of Portal Hypertension After Whipple, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.