NewYork-Presbyterian / Brooklyn Methodist Hospital Brooklyn, NY
Yash Bhagat, MD, Harsh Patel, MD, Saamia Faruqui, MD NewYork-Presbyterian / Brooklyn Methodist Hospital, Brooklyn, NY Introduction: Sevelamer carbonate is a non-absorbable phosphate-binding resin that is used to treat hyperphosphatemia in patients with chronic kidney disease. We highlight a case of Sevelamer initiation in a new hemodialysis (HD) patient that developed unremitting hematochezia with initial endoscopy finding prior to Sevelamer initiation of stercoral ulcerations and repeat biopsy post-initiation identifying new Sevelamer deposits.
Case Description/
Methods: A 63-year-old female admitted for a new diagnosis of nephrotic syndrome had her hospital course complicated by profuse hematochezia with a hemoglobin drop of 2 units (5.5 g/dL) from her baseline of 7.5 g/dL. A colonoscopy done at that time found erythematous mucosa in the rectum and a rectal ulcer. Biopsy of the rectum and rectal ulcer found surface erosion with reactive changes and necroinflammatory debris or fibrinopurulent exudates with reactive epithelial changes, respectively. These initial findings suggested that the patient's hematochezia was likely due to stercoral ulcerations. During the course of her hospitalization, the patient was started on Sevelamer carbonate for hyperphosphatemia. Fifteen days after Sevelamer initiation, the patient continued to have recurrent hematochezia requiring several blood transfusions and necessitating further exploration with a flexible sigmoidoscopy. The repeat procedure found diffusely friable ulcerated mucosa in the rectum near the dentate line with biopsies of the rectal ulcer revealing acutely inflamed granulation tissue associated with fragments of foreign body material suggestive of Sevelamer crystal resins. The patient’s Sevelamer was discontinued and she was started on rectal sucralfate enemas along with sennosides ultimately resulting in resolution of her lower gastrointestinal bleed (GIB). Discussion: Although a retrospective analysis of patients on HD has found no significantly increased risk of GIB in patients started on Sevelamer compared to non-Sevelamer phosphate binders, several individual cases of GIB have identified Sevelamer deposits in biopsied lesions. Our case suggests that rather than being the cause of GIB, Sevelamer deposition may aggregate at sites of mucosal erosion and cause recurrent bleeds in predisposed individuals. Further correlative evidence and systematic reviews are necessary to explore the exact role of Sevelamer in causing GIB.
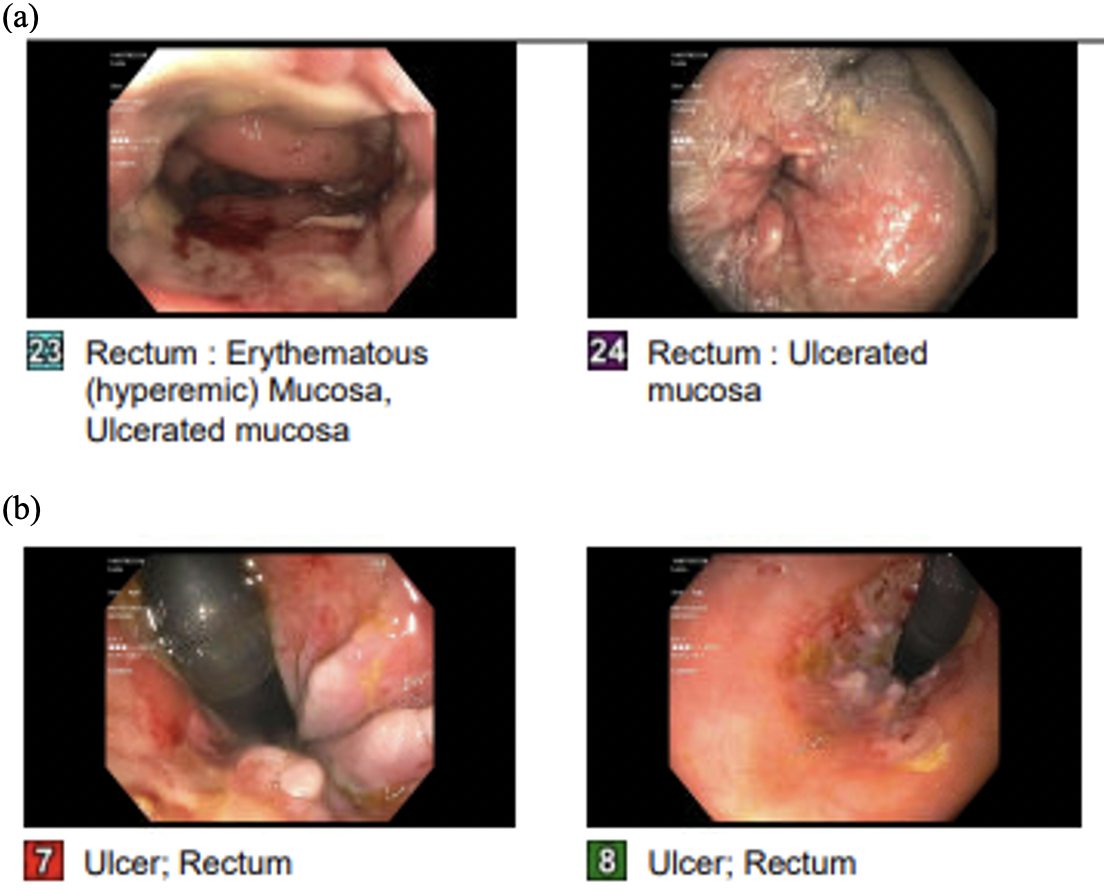
Figure: Figure 1: View on colonoscopy and flexible sigmoidoscopy of the rectal ulcer with no Sevelamer deposits prior to Sevelamer initiation (a) and after recurrent bleeding with biopsy-proven Sevelamer deposits 15 days after Sevelamer initiation (b).
Disclosures: Yash Bhagat indicated no relevant financial relationships. Harsh Patel indicated no relevant financial relationships. Saamia Faruqui indicated no relevant financial relationships.
Yash Bhagat, MD, Harsh Patel, MD, Saamia Faruqui, MD. P3097 - Rectal Sevelamer Deposits: An Irritant Causing Recurrent Lower Gastrointestinal Bleeds, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")