P3095 - Downhill Esophageal Variceal Hemorrhage Secondary to Superior Vena Cava Obstruction in a Patient with End-Stage Renal Disease: A Rare and Under-recognized Complication
University of Miami/Jackson Memorial Hospital Miami, FL
Award: ACG Presidential Poster Award
Keri-Ann Buchanan-Peart, MD1, Ritika Modi, 2, Gabriel Perreault, MD, MSc2, Joshua A. Turkeltaub, MD3, Sean Bhalla, MD2 1University of Miami/Jackson Memorial Hospital, Miami, FL; 2University of Miami Miller School of Medicine, Miami, FL; 3University of Miami Miller School of Medicine, Doral, FL Introduction: Downhill esophageal varices, a rare cause of upper gastrointestinal (GI) bleeding, are distinct from portal hypertensive varices in etiology, location, and treatment. They result from superior vena cava (SVC) obstruction, often due to malignancy, vascular devices, or central venous stenosis in hemodialysis patients. This case report highlights this phenomenon and the need for consideration in at-risk populations.
Case Description/
Methods: A 79-year-old male with end-stage renal disease (ESRD) on intermittent hemodialysis via a right internal jugular tunneled catheter presented with melena and large-volume hematemesis. He had no history of liver disease. Esophagogastroduodenoscopy (EGD) and colonoscopy done 18 months prior were normal.
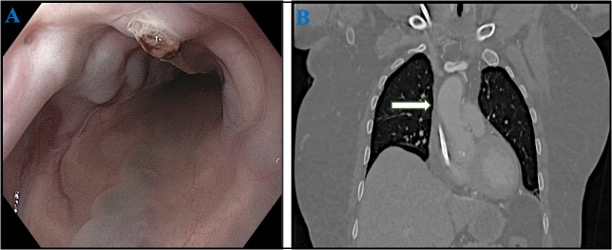
On presentation, he was hypotensive and tachycardic with hemoglobin 6.9 g/dL (baseline 10.3 g/dL), which improved with blood transfusion. Coagulation and liver tests were normal. Emergent EGD revealed three columns of large ( >5 mm) proximal esophageal varices (25–27 cm from incisors), one with a white nipple sign. (Figure 1) No distal esophageal varices or portal hypertensive gastropathy were seen. Endoscopic variceal ligation achieved hemostasis. Given the variceal location and absence of portal hypertensive gastropathy, a diagnosis of downhill esophageal varices was made.
Cross-sectional imaging revealed no signs of cirrhosis or portal hypertension. Chest CT showed non-opacification of the distal SVC between the right atrium and azygos vein, with prominent collateral vessels, suggesting chronic SVC stenosis. Venography confirmed occlusion at the bilateral brachiocephalic veins and SVC. Serial balloon venoplasty restored patency and central venous flow. He was discharged with a plan for follow-up EGD. Discussion: Downhill varices result from SVC obstruction and are found in the upper/mid esophagus, unlike portal hypertension-associated varices in the distal esophagus. Repeated central venous catheterization in ESRD contributes to central venous stenosis, as in this case. Despite this risk, downhill varices are underreported, likely due to subclinical presentations. Endoscopy aids diagnosis and temporizes bleeding via band ligation until definitive management involving endovascular recanalization restores central venous flow and reduces the risk of recurrent bleeding.
Downhill varices should be considered in ESRD patients with indwelling catheters and upper GI bleeding. Early recognition and targeted management are essential for optimal outcomes.
Figure: Figure 1. A: Upper endoscopy showing proximal esophageal varices and a white nipple sign. B: Coronal Chest CT showing non-opacification of the distal SVC (white arrow).
Disclosures: Keri-Ann Buchanan-Peart indicated no relevant financial relationships. Ritika Modi indicated no relevant financial relationships. Gabriel Perreault indicated no relevant financial relationships. Joshua Turkeltaub indicated no relevant financial relationships. Sean Bhalla indicated no relevant financial relationships.
Keri-Ann Buchanan-Peart, MD1, Ritika Modi, 2, Gabriel Perreault, MD, MSc2, Joshua A. Turkeltaub, MD3, Sean Bhalla, MD2. P3095 - Downhill Esophageal Variceal Hemorrhage Secondary to Superior Vena Cava Obstruction in a Patient with End-Stage Renal Disease: A Rare and Under-recognized Complication, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.