Dignity Health Saint Rose Dominican Las Vegas, Nevada
Shazia Pathan, MD1, Matthew Glover, MD2 1Dignity Health Saint Rose Dominican, Las Vegas, NV; 2Comprehensive Digestive Institute of Nevada, Las Vegas, NV Introduction: While milder GI symptoms have been independently reported with both infectious mononucleosis (IM) and excessive energy drink consumption, the following is a rare case of severe, biopsy-confirmed gastritis temporally linked to excess energy drink intake, following a recent diagnosis of IM.
Case Description/
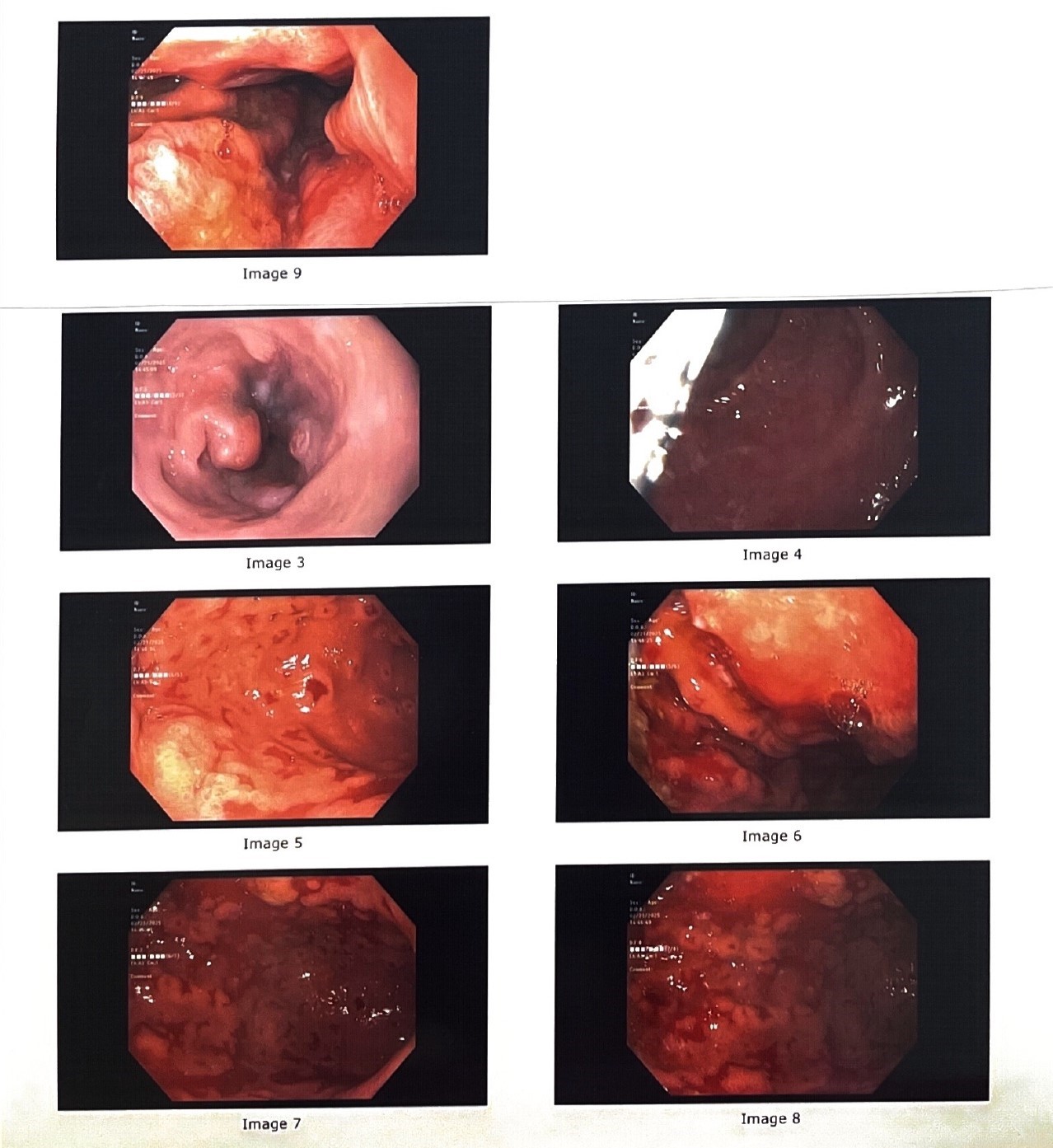
Methods: 23yoM presented with a few weeks onset of emesis, abdominal discomfort. Upon admission, labs are significant for elevated LFTs, hypocalcemia, severely low vitamin D level, elevated PTH, and hypoalbuminemia. He was also diagnosed with EBV+ IM (positive Monospot test and significantly elevated EBV VCA IgG levels). CT abdomen/pelvis, MRCP were unrevealing. EGD found severe esophagitis and gastroduodenitis with erosion of many portions of the gastric body lumen. Biopsies confirmed marked reflux-associated changes in esophagus; atypical gastric mucosa with acute erosive changes, focal lamina propria changes suggestive of healing ulcer; acute on chronic erosive duodenitis. No H. pylori. The patient denied alcohol, NSAID, smoking, & other illicit drug use. On further laboratory work up: B12, gastrin, HIV, GPC Ab- IgG, LKM-1 Ab IgG, ceruloplasmin, VIP, all other viral/bacterial PCR were normal or negative. The only notable history was the patient's chronic energy drink intake of ~5 drinks per day. The patient was prescribed PPI and advised energy drink cessation, with plans to repeat EGD with Sydney Protocol. At 4-week follow-up, GI symptoms had resolved, LFTs normalized. Discussion: The lab findings alone point toward chronic malabsorption, rather than an isolated acute EBV infection. The acute-on-chronic histologic changes on biopsy suggest that the combination of preexisting inflammation— worsened by a systemic viral illness—and repeated irritation from ongoing stimulant consumption likely exacerbated the severity of the gastritis. Energy drinks, which contain high levels of caffeine, taurine, citric acid, are known to stimulate gastric acid secretion, delay emptying, and disrupt mucosa. Atypia on biopsy without lymphocytic infiltration reflects chemical irritation rather than viral effect and posits that stimulant exposure was the primary driver of the clinical presentation.
This case highlights the diagnostic challenge of distinguishing between viral and chemically induced gastric injury. It also underscores a shift- to rank energy drink toxicity higher among differentials for severe gastritis—particularly in younger patients, among whom ~60% may consume energy drinks daily.
Figure: Figure 1
Disclosures: Shazia Pathan indicated no relevant financial relationships. Matthew Glover indicated no relevant financial relationships.
Shazia Pathan, MD1, Matthew Glover, MD2. P3013 - Monster Burn: Severe Gastritis Following Acute Mononucleosis in the Setting of Excess Energy Drink Consumption, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")