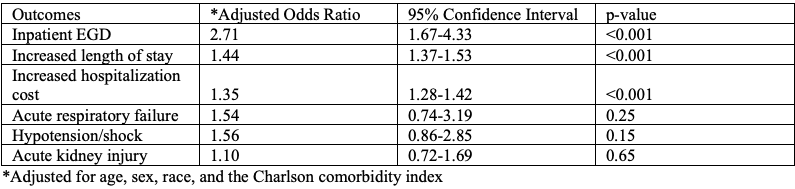
Alexander J. Kaye, MD, MBA1, Narinderjeet Kaur, MD, MS2, Kariana Martinez, MD2, Anwar Uddin, MD2, Elizabeth Kaye, AB3, Bani Chander-Roland, MD4, Daniel DiLeo, MD4 1SUNY Downstate Health Sciences University, Staten Island, NY; 2SUNY Downstate Health Sciences University, Brooklyn, NY; 3McLean Hospital, Boston, MA; 4Brooklyn VA Medical Center, Brooklyn, NY Introduction: Hyperemesis gravidarum (HG) is a common reason for hospitalization in pregnant patients in their first and second trimesters. In severe forms, HG may lead to elective termination of wanted pregnancies and cause fetal growth restriction. Constipation is a highly prevalent syndrome impacting up to 38% of pregnant women. Constipation in prior studies has shown to increase length of stay (LOS) and increase mortality rates. However, this relationship is best established in older populations. Despite the prevalence of constipation and severity of HG, there is a paucity of literature exploring their relationship. Our study aim is to understand the impact of comorbid constipation on the outcomes of hospitalized women with HG. Methods: Hospitalized women diagnosed with HG were selected from the 2020 National Inpatient Sample database. ICD-10 codes were used to select diagnoses. Demographic data and outcomes of HG were compared between a subgroup with constipation, and without constipation. The outcomes of interest were length of stay (LOS), hospitalization cost, hypotension/shock, acute kidney injury (AKI), acute respiratory failure, and inpatient EGD. Chi-squared tests and independent t-tests were used to compare proportions and means respectively. A multivariate logistic regression analysis was used to establish if constipation is an independent predictor for the outcomes after adjusting for age, race, and Charlson Comorbidity Index (CCI). Results: For the year 2020, 135,005 hospitalized adults were diagnosed with HG. Patients with HG and comorbid constipation were less likely to be white (31% vs 39%, p< 0.001). All patients were female and there was no significant difference in age (27.2 years old vs. 27.2 years old, p=0.782). Constipation was an independent risk factor for inpatient EGD (adjusted odds ratio (aOR) 2.71, 95% confidence interval (CI): 1.67-4.33, p< 0.001), increased LOS (4.4 days vs. 3.0 days, aOR 1.44, 95% CI: 1.37-1.53, p< 0.001), and increased hospitalization cost ($7,492 vs. $5,445, aOR 1.35, CI 1.28-1.42, p< 0.001). Constipation was not a risk factor for AKI (p=0.65), acute respiratory failure (p=0.25), and hypotension/shock (p=0.15). Discussion: In hospitalized women with HG, constipation is a risk factor for inpatient EGD, increased LOS, and increased hospitalization cost. Further randomized prospective trials would be beneficial to further explore the relationship between HG and constipation and whether improved constipation prophylaxis would help mitigate these outcomes.
Figure: Multivariate logistic regression analysis of clinical outcomes among hyperemesis gravidarum with comorbid constipation
Disclosures: Alexander Kaye indicated no relevant financial relationships. Narinderjeet Kaur indicated no relevant financial relationships. Kariana Martinez indicated no relevant financial relationships. Anwar Uddin indicated no relevant financial relationships. Elizabeth Kaye indicated no relevant financial relationships. Bani Chander-Roland indicated no relevant financial relationships. Daniel DiLeo indicated no relevant financial relationships.
Alexander J. Kaye, MD, MBA1, Narinderjeet Kaur, MD, MS2, Kariana Martinez, MD2, Anwar Uddin, MD2, Elizabeth Kaye, AB3, Bani Chander-Roland, MD4, Daniel DiLeo, MD4. P2949 - Outcomes of Patients Hospitalized for Hyperemesis Gravidarum with Comorbid Constipation, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")