
Monday Poster Session
Category: Endoscopy Video Forum
 photo")
Preeyati Chopra, MBBS (she/her/hers)
Mayo Clinic
Hartford, CT
Chronic inflammation in Crohn’s Disease (CD) has a relapsing course and can progress to stricturing phenotype, penetrating phenotype or both. More than half of the CD patients develop intestinal complications significantly impacting their quality of life. Patients present with abdominal pain, cramping and obstruction. Common treatment modalities for CD-related fistulas include medical management (effective in < 50% of patients) and surgery which is more invasive and carries risk for operative adverse events. We describe endoscopic myotomy for the management of ileo-colo-cecal fistula.
Case Description/
Methods:
A 45-year-old male with CD status post end colostomy and abdominoperineal resection presented with abdominal pain and obstructive symptoms. CT showed discontinuous areas of chronic inflammation around the terminal ileum and ileocecal valve (ICV). Colonoscopy revealed moderate stenosis at the level of the ICV and terminal ileum (traversed after dilation up to 15mm), inflammation and ulceration in the terminal ileum with a Simple Endoscopic Score for CD (SES-CD) aggregate score of 7. The patient was started on risankizumab and planned for repeat imaging and colonoscopy in 6 months. Despite the dilation, the patient continued to experience obstructive symptoms. Repeat imaging showed enhancing tracts from the base of appendix to the inflamed terminal ileum with luminal narrowing.
On repeat colonoscopy, a complex ileo-colo-cecal fistula was seen along with a bridge containing circular muscle plugging the ICV with distension of the gut proximal to the ICV (figure 1). The decision was made to deroof it. A flexible tip guidewire was used to delineate the muscular bridge from the lumen. Using endoscopic scissors, a circumferential incision was made around the lesion into the submucosa and the muscle band. Two hemostatic clips were placed after cutting to prevent post-intervention bleeding (figure 2A, 2B). Moderate stenosis measuring 5 cm X 1.2 cm was noted again at the terminal ileum and dilated up to 15 mm.
On follow-up imaging, the patient was noted to have stable chronic inflammation. Follow-up colonoscopy showed mild segmental inflammation correlating to his history. His obstructive symptoms are under control after his de-roofing procedure, and he is on maintenance risankizumab.
Discussion:
With no definitive management for fistulas in CD patients, we highlight endoscopic myotomy as a minimally invasive technique with high effectiveness in the treatment of this condition.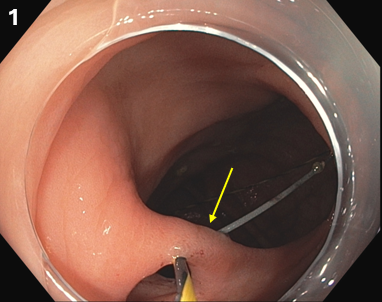
Figure: 1: A tissue bridge containing circular muscle plugging the Ileo-Cecal valve (arrow)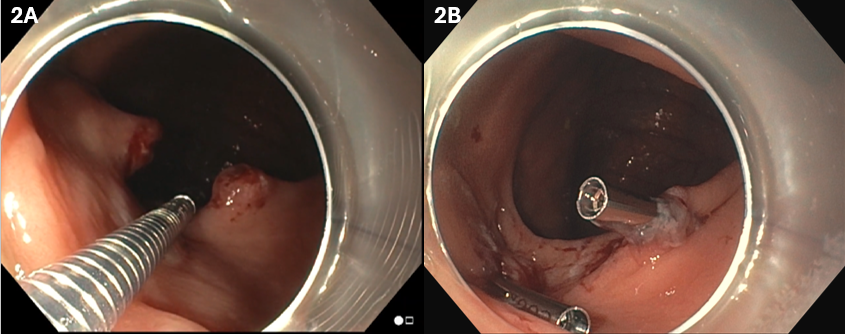
Figure: 2A: Endoscopy: Tissue Bridge after being cut with endoscopic scissors
2B: Endoscopy: Hemostatic clips placed after cutting the band
Disclosures:
Preeyati Chopra indicated no relevant financial relationships.
Mayank Goyal indicated no relevant financial relationships.
Ashwariya Ohri indicated no relevant financial relationships.
Navtej Buttar indicated no relevant financial relationships.
Preeyati Chopra, MBBS1, Mayank Goyal, MBBS2, Ashwariya Ohri, MBBS3, Navtej Buttar, MD2. P2723 - A Cut Above: Endoscopic Myotomy of an Ileo-Colo-Cecal Fistula in Crohn’s Disease, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.