Case Western Reserve University / MetroHealth Cleveland, OH
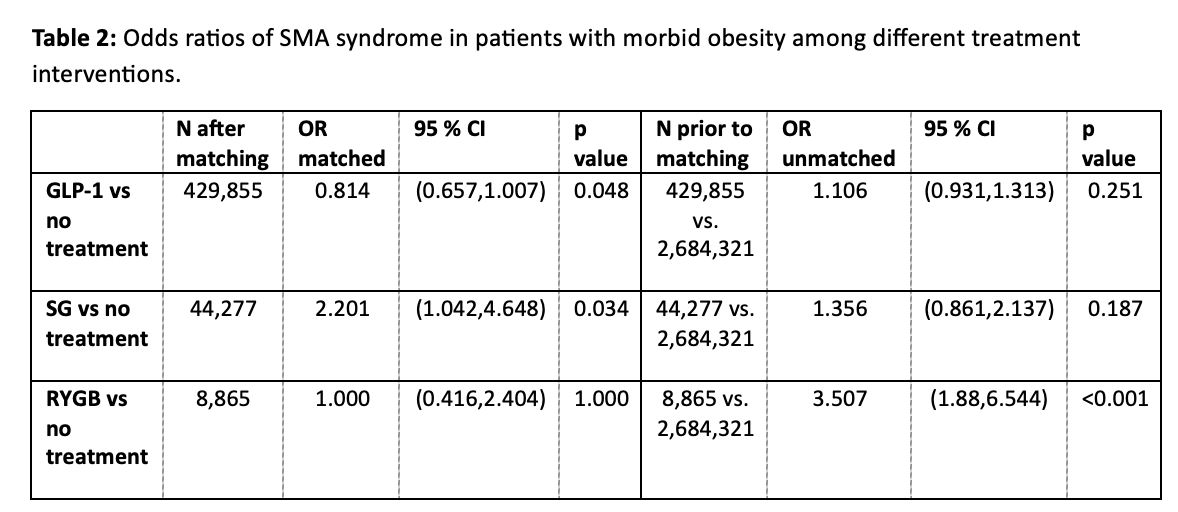
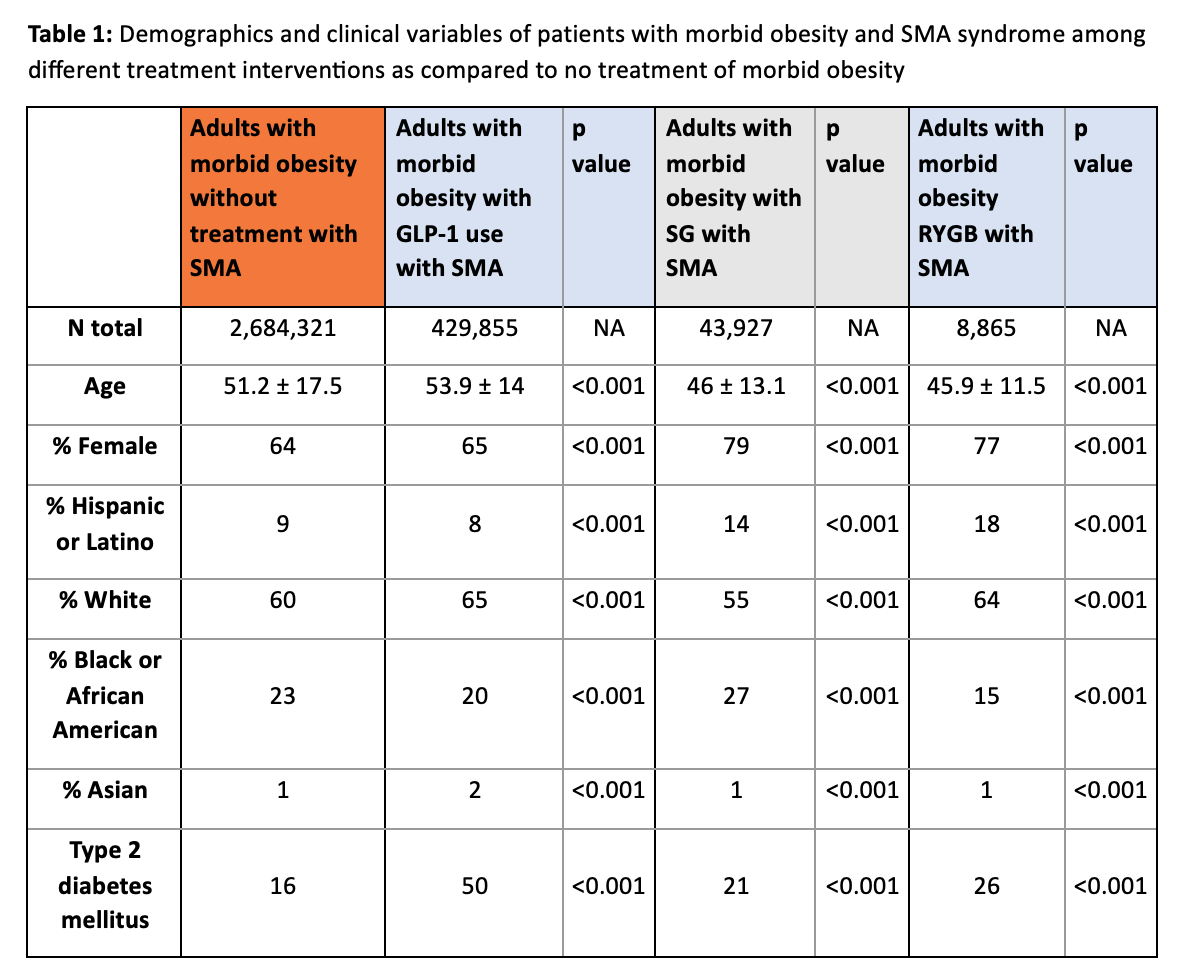
Alexander Malik, MD1, Thai Hau Koo, MD2, Raj Shah, MD3, Michael Kurin, MD1 1Case Western Reserve University / MetroHealth, Cleveland, OH; 2University of Sciences Malaysia Specialist Hospital, Kelantan, Kelantan, Malaysia; 3The Ohio State University Wexner Medical Center, Columbus, OH Introduction: Therapies for morbid obesity including bariatric surgery (BS) and glucagon-like peptide (GLP-1) agonists frequently result in rapid weight loss. Superior mesenteric artery syndrome (SMAS) may occur due to rapid weight loss, though the association between weight loss therapy and SMAS has not been fully elucidated. We aimed to determine the prevalence of SMAS in patients who received therapies for morbid obesity. Methods: We conducted a retrospective cohort study using de-identified patient data from the global TriNetX database (2021-2024). Adults with class 3 obesity (BMI >40) were included and divided into four cohorts: Untreated morbid obesity (UMO), morbid obesity treated with a GLP-1 agonist, sleeve gastrectomy (SG), or roux en Y gastric bypass (RYGB). Propensity score matching (PSM) was used to adjust for confounding factors. Kaplan-Meier and univariate Cox proportional hazards models were used to assess the prevalence of SMAS at 12 months. Subgroup analyses included prevalence of SMAS in patients with class 1-2 obesity (BMI 30-39.9) treated with GLP-1 agonists versus patients with untreated class 1-2 obesity (UO). Results: The database contained 3,165,216 adults with morbid obesity during the study period; 429,855 treated with GLP-1 agonists, 43,927 with SG, 8,865 with RYGB, and 2,630,282 untreated. SMAS was diagnosed in 2,229 patients (92 GLP-1 group, 15 SG, 10 RYGB and 2,112 untreated). After PSM, treatment with a GLP-1 agonist showed a non-statistically significant negative association with SMAS compared to UMO (OR 0.81; 95% CI 0.66,1.01; p 0.048). SG showed significant association with SMAS compared to UMO (OR 2.20, 95% CI 1.04,4.65, p 0.03) (Table 2); the RYGB cohort did not show a significant association. There were 10,892,032 patients with class 1-2 obesity; 751,830 were treated with GLP-1 agonists. Odds of SMAS were decreased in this group compared to UO (OR 0.80, 95% CI 0.69,0.93, p 0.003). Discussion: Based on a large global dataset, the prevalence of SMAS in patients with morbid obesity is exceedingly low and the prevalence is decreased in patients treated with GLP-1 agonists or BS compared to patients with UMO. The reason for this result requires further explanation but may suggest the increased risk of SMAS with rapid weight loss only occurs in patients who become underweight. Our findings do not suggest there is a need for clinicians to counsel patients considering weight loss therapy on risks of SMAS.
Figure: Table 1: Demographics and clinical variables of patients with morbid obesity and SMA syndrome among different treatment interventions as compared to no treatment of morbid obesity
Figure: Table 2: Odds ratios of SMA syndrome in patients with morbid obesity among different treatment interventions
Disclosures: Alexander Malik indicated no relevant financial relationships. Thai Hau Koo indicated no relevant financial relationships. Raj Shah indicated no relevant financial relationships. Michael Kurin indicated no relevant financial relationships.
Alexander Malik, MD1, Thai Hau Koo, MD2, Raj Shah, MD3, Michael Kurin, MD1. P2691 - Examining the Associations Between Treatments for Morbid Obesity and Superior Mesenteric Artery Syndrome, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Alexander Malik, MD photo")