Suhail Sidhu, MD1, Shoujit Banerjee, MD1, Daniel Mai, MD1, Nicholas N. Totah, MD2, Yuri Kwon, MD2, Frances Dang, MD, MSc3, Peter Nguyen, MD1, Gregory Albers, MD, FACG4 1University of California Irvine, Orange, CA; 2University of California Irvine Health, Orange, CA; 3University of California Irvine, Irvine, CA; 4University of California Irvine Digestive Health Institute, Orange, CA Introduction: Lynch Syndrome (LS), also known as hereditary nonpolyposis colorectal cancer (HNPCC), is the most common inherited form of colon cancer. LS is due to an autosomal dominant mutation in mismatch repair genes, which causes increased microsatellite instability leading to increased risk for colonic and noncolonic tumors. Colonoscopy plays a pivotal role in preventing, diagnosing, and treating colon cancer. This case report underscores the importance of adhering to strict colorectal cancer (CRC) surveillance in patients with LS, even with multiple reassuring colonoscopies.
Case Description/
Methods: A 53-year-old male with a history of LS (MSH2) mutation, ADHD, MDD, and alcohol use disorder presented for routine biennial colonoscopy surveillance. Colonoscopy three years ago was unremarkable, and colonoscopies from five and six years prior revealed multiple flat and sessile polyps >1cm, which were found to be noncancerous. At the time of his surveillance colonoscopy, for which he was 18 months overdue, the patient was asymptomatic, denying changes in bowel habits, bleeding, fever, weight loss, or night sweats. During the procedure, a 1 cm bi-lobed polyp was identified in the fold of the sigmoid colon at 35cm. Polypectomy was performed with good post-resection margins. Pathology later revealed poorly differentiated adenocarcinoma, at least intramucosal, arising from background of tubular adenoma. One month after diagnosis, the patient underwent laparoscopic total colectomy with ileorectal anastomosis, partial omentectomy, and flexible sigmoidoscopy. CT scan four months after surgery revealed no evidence of cancer recurrence. Discussion: In patients diagnosed with Lynch Syndrome, CRC surveillance is recommended every one to two years beginning at ages 20-25 or two to five years prior to diagnosis of CRC in a family member. Our patient with LS who missed his surveillance colonoscopy by 18 months was ultimately diagnosed with CRC and required total colectomy thereafter. In patients with LS who undergo colectomy, surveillance colonoscopies are recommended every one to two years. This case highlights the importance of maintaining strict CRC surveillance intervals for early detection of CRC in patients with Lynch syndrome.
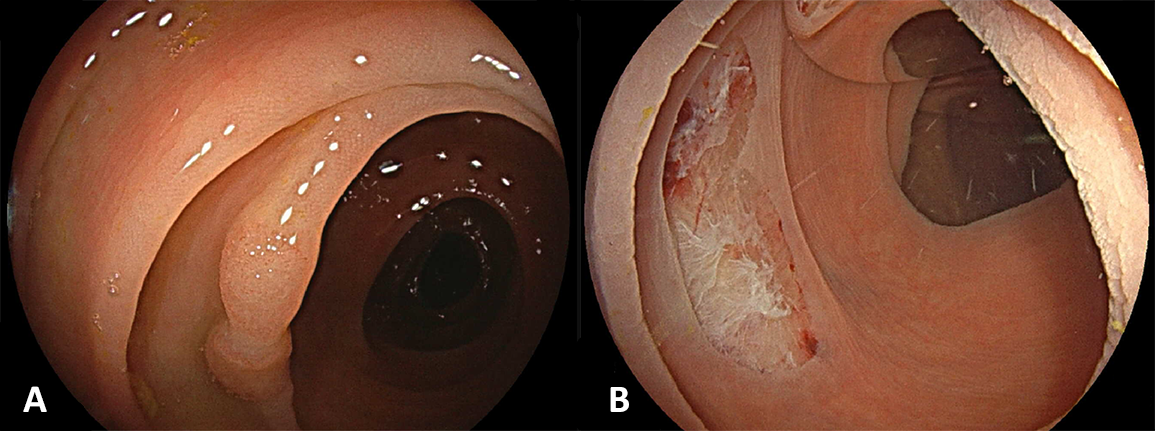
Figure: Figure 1. One cm bi-lobed polyp in the sigmoid colon revealing poorly differentiated adenocarcinoma (A). Post polypectomy site with good post-resection margins (B).
Disclosures: Suhail Sidhu indicated no relevant financial relationships. Shoujit Banerjee indicated no relevant financial relationships. Daniel Mai indicated no relevant financial relationships. Nicholas Totah indicated no relevant financial relationships. Yuri Kwon indicated no relevant financial relationships. Frances Dang: Cook Medical – Speaker. Peter Nguyen indicated no relevant financial relationships. Gregory Albers indicated no relevant financial relationships.
Suhail Sidhu, MD1, Shoujit Banerjee, MD1, Daniel Mai, MD1, Nicholas N. Totah, MD2, Yuri Kwon, MD2, Frances Dang, MD, MSc3, Peter Nguyen, MD1, Gregory Albers, MD, FACG4. P2677 - Colonoscopy Surveillance Remains the Lynchpin in Management of Lynch Syndrome, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.