The Warren Alpert Medical School of Brown University Warwick, RI
Gurjot Singh, DO1, Celinie Nguyen, 2, Muhammad Ali, MBChB1, Tamara Koritarov, DO, MSc3, Kyle Rollheiser, MD4 1The Warren Alpert Medical School of Brown University, Warwick, RI; 2Warren Alpert Medical School of Brown University, Providence, RI; 3Kent Hospital, Providence, RI; 4Warren Alpert Medical School of Brown University, Warwick, RI Introduction: Large bowel obstructions are an uncommon form of pathology found within the intestinal tract. An even rarer form of large bowel obstruction is a case of cecal bascule that we present in a patient undergoing thoracic surgery for a spiculated lung nodule, whose course was also complicated by septic shock from peritonitis caused by bowel perforation.
Case Description/
Methods: A 74-year-old man with history of type 2 diabetes, coronary artery disease status, and an extensive smoking history was referred to thoracic surgery for VATS resection later converted to open thoracotomy for an abnormal nodule. On post-op day (POD) 2 the patient exhibited epigastric tenderness, abdominal distension and discomfort, without flatus or vomiting. Abdominal x-ray demonstrated multiple loops of distended small and large bowel, with bowel obstruction not completely excluded. An NG tube was placed. CT demonstrated diffusely distended small bowel loops, and sigmoid diverticulitis with stool-filled right lower quadrant viscus in sigmoid or cecum suspicious for adynamic ileus. On POD8, the patient was febrile to 39°C, distended, with no bowel movements. An abdominal x-ray was obtained with findings of a new significantly dilated and inverted cecum from 10 to 14 cm in diameter, suggestive of cecal bascule with stable dilated loops of small bowel. An exploratory laparoscopy revealed the cecum folding from its lower portion superomedially towards the left upper quadrant, confirming a cecal bascule with feculent peritonitis and perforation with a 6-inch rent along the anterior aspect. Subsequently, a right colectomy and creation of end ileostomy and transverse colon fistula, with peritoneal lavage was performed. Postoperative antibiotics and antifungal coverage was started. The patient was stabilized and discharged to a skilled nursing facility. Discussion: Large bowel obstructions are less common compared to small bowel obstructions. Within the minority subset of large bowel obstruction, an even rarer form is known as a cecal bascule. A cecal volvulus involves the torsion of the cecum around its mesentery versus a bascule which involves the upward folding of the cecum without any mesenteric involvement. A cecal bascule is difficult to diagnose and can initially present as non-specific pain. An untreated bascule can lead to rapid distension and peritonitis, a complication observed in this case. Overall, this case highlights the importance of rare diagnosis which can lead to serious complications if undiagnosed.
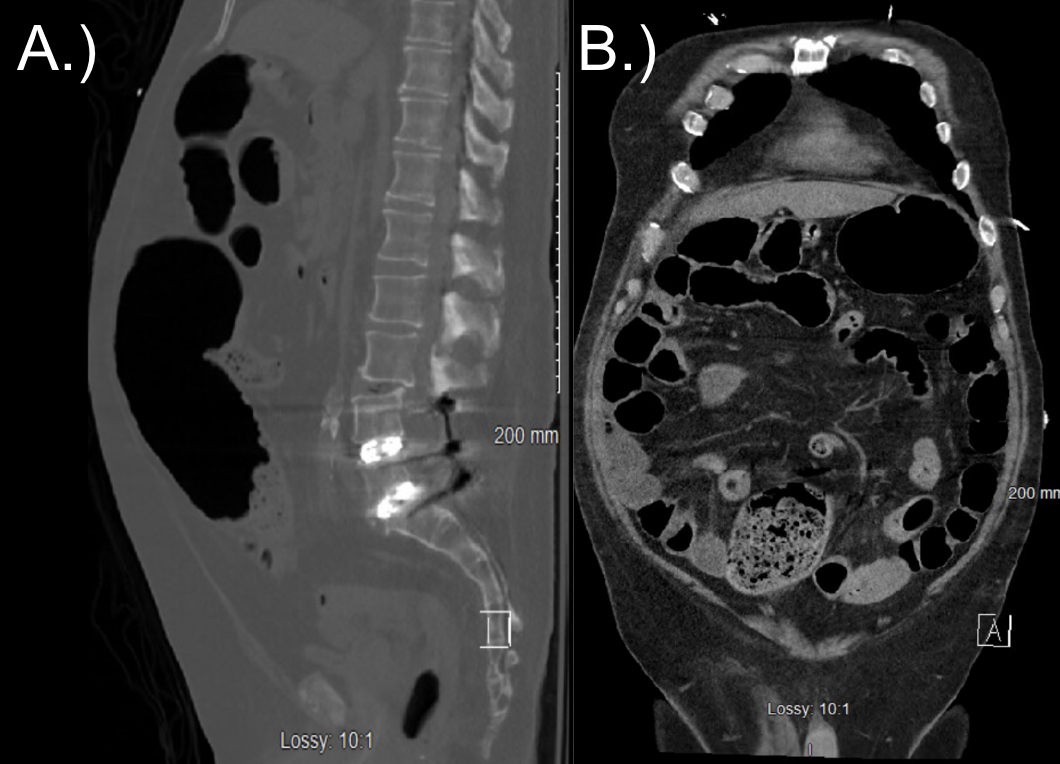
Figure: Sagittal (A.) and Coronal (B.) of CT Abdomen/Pelvis on POD5. Multiple loops of fluid-filled small bowel without focal point of obstruction. Acute diverticulitis of the sigmoid colon. No perforation noted.
Figure: KUB on POD8. Multiple dilated loops of small bowel with significant dilatation and inversion of the cecum, suggestive of a cecal bascule.
Disclosures: Gurjot Singh indicated no relevant financial relationships. Celinie Nguyen indicated no relevant financial relationships. Muhammad Ali indicated no relevant financial relationships. Tamara Koritarov indicated no relevant financial relationships. Kyle Rollheiser indicated no relevant financial relationships.
Gurjot Singh, DO1, Celinie Nguyen, 2, Muhammad Ali, MBChB1, Tamara Koritarov, DO, MSc3, Kyle Rollheiser, MD4. P2529 - A Twisted Tale: The Unraveling of a Cecal Bascule, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.