
Monday Poster Session
Category: Colon

Matthew A. Kalloo, MD
Harlem Hospital Center
New York, NY
Müllerian tissues originate from paramesonephric ducts and differentiate into uterus, fallopian tubes, cervix, and upper vagina. Müllerian adenocarcinomas account for 2% of gynecologic neoplasms. GI metastases usually occurs to the rectosigmoid or rectovaginal septum. We report a case of Mullerian adenocarcinoma presenting as a large colonic mass.
Case Description/
Methods:
A 59-year-old female presented with 2 weeks of fatigue and abdominal pain. Her last menstrual period was 13 days ago. She was afebrile, BP 153/75, pulse 138. She was pale and lethargic with a benign nondistended abdomen. Hb was 4.6, MCV 68.8, WBC 9.9k, and platelets 498k. Ferritin was 18 ng/ml, iron 11 μg/dl, iron saturation 3%, Retics 3.28% and LDH 283 U/L. CT showed multiple cystic heterogeneous irregular abdominopelvic masses; in the area of the ovaries, adjacent to the uterus, LUQ, RUQ, and epigastric, most 5-10 cm, with multiple scattered pelvic, mesenteric, and inguinal lymph nodes. (Fig.1). She was admitted to ICU where she was transfused. EGD was normal. Colonoscopy showed a fungating, non-obstructive, non-bleeding, partially circumferential mass in the ascending colon, 20 cm in length (Fig. 2). Biopsy revealed a poorly differentiated adenocarcinoma of primary Müllerian origin. CA-125 was elevated at 2006 U/ml (< 38); CA 19-9 and CEA were both normal. She declined additional work up. She was discharged with Hb of 8.1. She presented 2 months later to an outside facility with multifocal small and large bowel obstruction due to peritoneal carcinomatosis. She was again offered surgery and chemotherapy but declined.
Discussion: Endometriosis is a risk factor for Müllerian adenocarcinomas. These cancers mostly occur in postmenopausal women (average age 66), and present with vaginal bleeding, abdominal pain and distension. It can mimic colorectal cancer with rectal bleeding, anemia, and mass effect from a rectosigmoid or rectovaginal mass. Spread is mostly hematogenous to the liver and lungs followed by lymphatic and direct spread. Colonic metastasis is rare. Surgical resection is the mainstay of treatment, with a role for adjuvant chemotherapy. Our patient’s presentation was atypical due to its size ( >4.2cm) and location. In addition, she was not strictly postmenopausal. The multiple cystic ovarian masses suggest occurrence in the setting of endometriosis. In conclusion, colonic adenocarcinoma of Mullerian origin can mimic primary colorectal cancer both clinically and endoscopically. 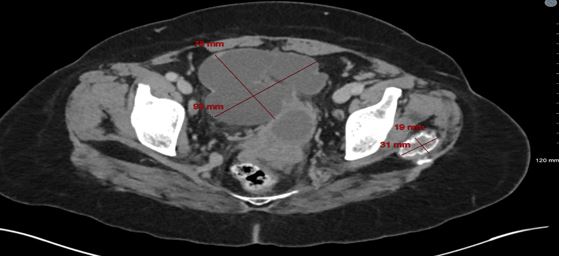
Figure: Fig.1 Multiple abdominopelvic masses 
Figure: Fig 2. Colonic mass
Disclosures:
Matthew Kalloo indicated no relevant financial relationships.
Mohamed Osman indicated no relevant financial relationships.
Geraldine Mould indicated no relevant financial relationships.
Peter Santogade indicated no relevant financial relationships.
Joan Culpepper-Morgan indicated no relevant financial relationships.
Matthew A. Kalloo, MD1, Mohamed K.. Osman, MD, MPH2, Geraldine K. Mould, MD1, Peter K. Santogade, MD, FACG1, Joan A.. Culpepper-Morgan, MD, FACG3. P2492 - Adenocarcinoma of Mullerian Origin Presenting as Giant Non-Obstructing Ascending Colonic Mass, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.