Staten Island University Hospital, Northwell Health Staten Island, NY
Toni Habib, MD1, Peter Mounas, DO2, Micaela Prisco, MSc1, Chloe Lahoud, MD1, Ali Sohail, DO3, Saif Yasin, DO1, Hassan Al Moussawi, MD1 1Staten Island University Hospital, Northwell Health, Staten Island, NY; 2Rowan-Virtua School of Osteopathic Medicine, Marlboro, NJ; 3Staten Island University Hospital, Northwell Health, Brooklyn, NY Introduction: Pancreatic signet ring cell carcinoma (PSRCC) represents an exceptionally aggressive subtype of pancreatic adenocarcinoma, typically marked by poor prognosis. This report details a case of PSRCC diagnosed within a phenomenally brief progression window, further complicating the already challenging early detection and management of pancreatic cancer.
Case Description/
Methods: A 50-year-old male presented to the emergency department reporting sudden and severe left and right lower quadrant abdominal pain. Accompanying symptoms included nausea, vomiting, and chills. The initial examination did not reveal any specific cause; however, a CT scan of the abdomen and pelvis conducted during this visit showed signs of sigmoid colitis without any noticeable pancreatic or liver abnormalities. The patient was treated with antibiotics for colitis and discharged with instructions for outpatient follow-up, which included a colonoscopy that subsequently showed no signs of malignancy. Despite initial treatment, the patient revisited the emergency department six weeks later with unresolved and intensified epigastric pain radiating to the back, divergent from his initial pain. This time, a repeat CT scan, revealed an ill-defined hypoattenuating area in the pancreatic body suggesting necrosis or a potential mass, and multiple new liver lesions indicative of metastases—significant findings absent in the earlier scans. An endoscopic ultrasound (EUS) was subsequently performed which identified a heterogeneous, irregular mass at the junction of the pancreatic body and tail, alongside evidence of liver metastasis. Fine needle biopsies were obtained from both the pancreatic mass and a liver lesion. The pathology confirmed infiltrating adenocarcinoma of the pancreatic tail with focal signet ring cell-like features. Following the diagnosis, the patient was referred to oncology for further management. Discussion: This case underscores the aggressive nature of PSRCC and the limitations of standard imaging techniques in early detection. The rapid evolution from an unremarkable initial CT scan to widespread metastatic disease highlights the need for heightened clinical vigilance in atypical abdominal pain cases.
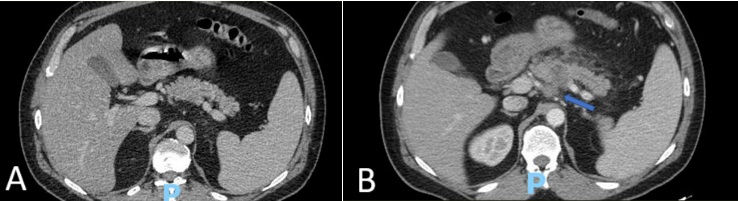
Figure: Initial CT showing normal pancreatic body/ tail junction (A), compared with the repeat CT 6 weeks later showing pancreatic mass at the body/ tail junction (B)
Figure: Endoscopic ultrasound image showing the pancreatic mass at the body/ tail junction.
Disclosures: Toni Habib indicated no relevant financial relationships. Peter Mounas indicated no relevant financial relationships. Micaela Prisco indicated no relevant financial relationships. Chloe Lahoud indicated no relevant financial relationships. Ali Sohail indicated no relevant financial relationships. Saif Yasin indicated no relevant financial relationships. Hassan Al Moussawi indicated no relevant financial relationships.
Toni Habib, MD1, Peter Mounas, DO2, Micaela Prisco, MSc1, Chloe Lahoud, MD1, Ali Sohail, DO3, Saif Yasin, DO1, Hassan Al Moussawi, MD1. P2316 - A Case of Highly Aggressive Signet Ring Cell-Like Pancreatic Cancer, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.