Anni Chowdhury Arellanes, DO1, Montserrat Guraieb Trueba, MD1, Van Karlyle II Morris, MD1, Phillip S.. Ge, MD2, Emmanuel Coronel, MD2 1MD Anderson Cancer Center, Houston, TX; 2The University of Texas MD Anderson Cancer Center, Houston, TX Introduction: Immunotherapy (ICI) with programmed death 1blockade such as pembrolizumab hasbeen efficacious intreating early-stage deficient DNA mismatch repair (dMMR) and microsatellite instability-high (MSI-H) colorectal tumors. Interestingly, this therapy has been reported to cause significant regression of colorectal cancer.Here we report acaseof an elderly patient withlocally invasivecolon cancer(T3N0M0), that was treated with pembrolizumab andendoscopic submucosal dissection.
Case Description/
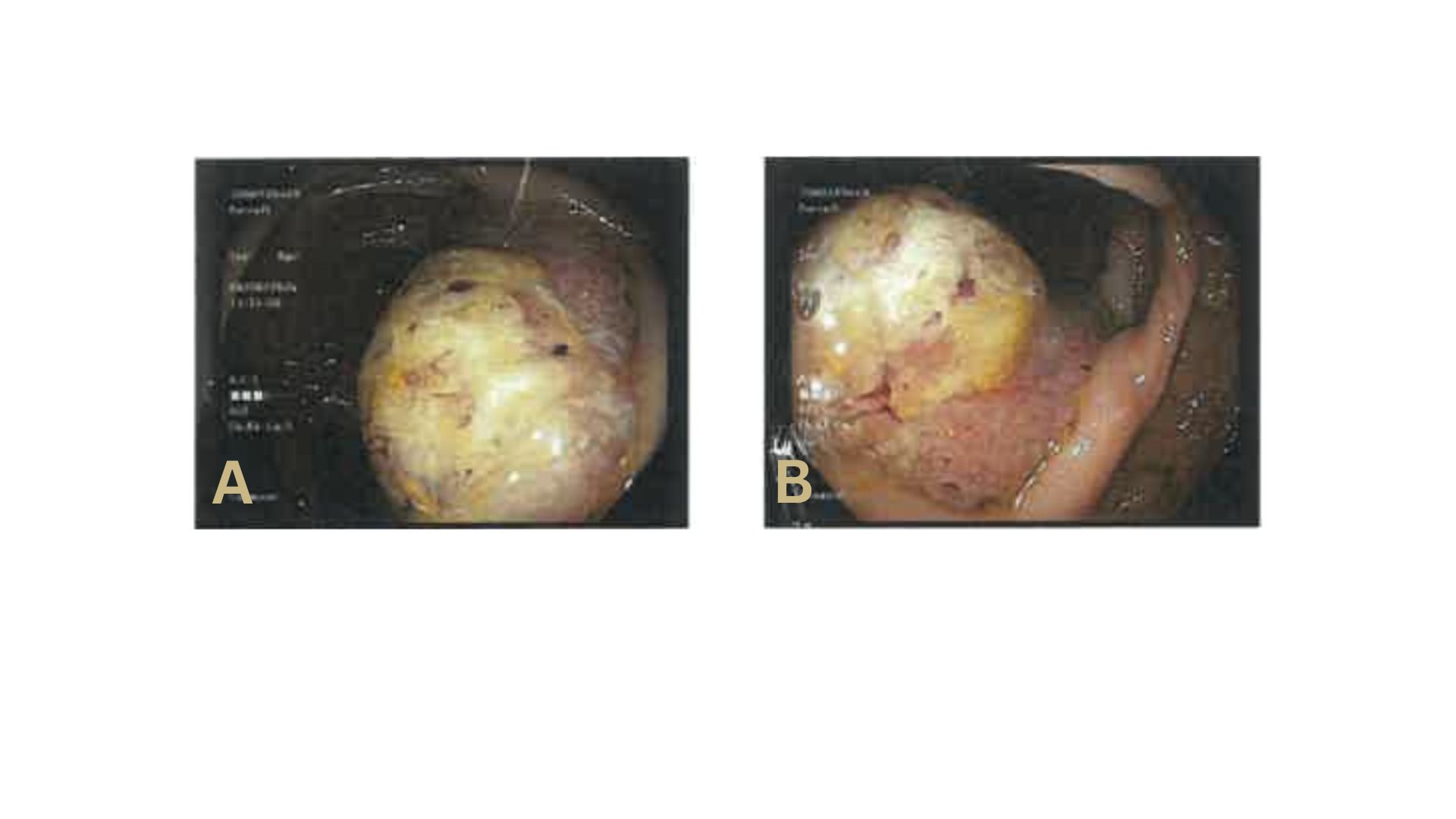
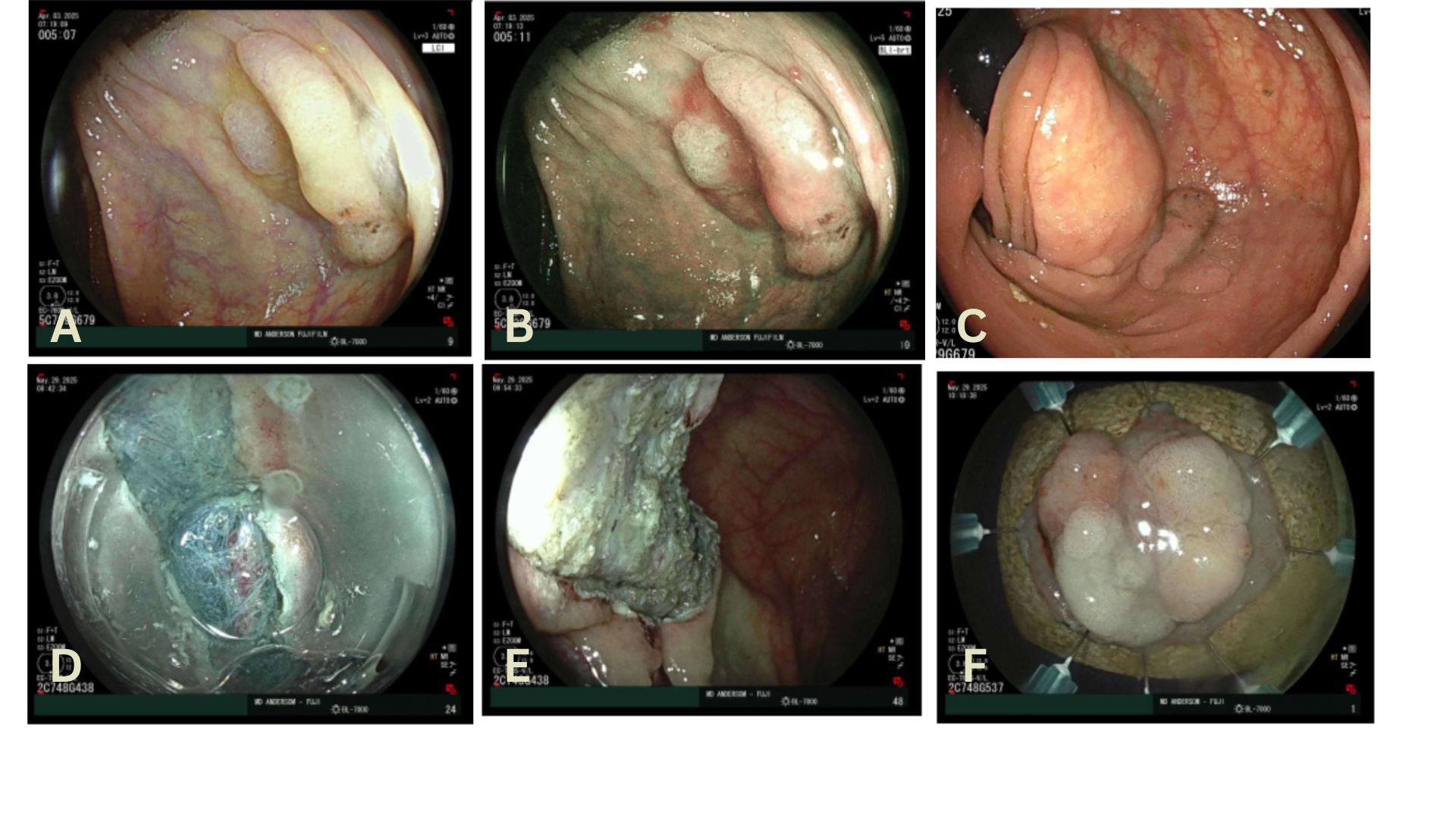
Methods: 88M with medical history of hypertension, atrial fibrillation with pacemaker and multiple colonic polyps since index colonoscopy at age 58.Surveillance colonoscopy on 6/6/24 found a 3cmfriable ascending colon mass with pathology confirming invasive moderately differentiated adenocarcinoma, MSI-H with loss of MLH1 and PMS2. Hestarted on first line treatment with single agent pembrolizumab on 8/7/2024. Within 2 months, there wasa decrease in size of the lesion from 3cmto 1.9cmandno increase in size or evidence of metastasis at 8 months. Colonoscopyperformedto assess treatment response showed a polypoid non-obstructing 3cmascending colon mass withan adjacent tattoo.Biopsies revealed sessile serrated lesion with high grade dysplasia and no malignancy noted. The case was discussed at multidisciplinary tumor board and since he was not a surgical candidate, the decision was made to attempt endoscopic resection. Theresidual masswas then resected successfully with endoscopic submucosal dissection (ESD). A 4cm by 4cmresection specimen was obtained; the specimen was removed en-bloc. (Figure 2).The margins were free of polypoid tissue. Pathology showed minute focus of invasive adenocarcinoma without evidence of lymphovascular invasion. Discussion: dMMR & MSI-H tumors account for 15% of all colorectal cancers.Immunotherapy has the potential to change the standard of care for localized dMMRtumorsas it has shown high rates of pathologic, radiographic, and endoscopic response. As a result, organ-sparing strategies including endoscopic resection with ESD are becomingfeasiblemanagement optionsfor these lesions that previouslyrequired invasive surgical resection.
Figure: Figure 1. 3cm Right Colon Mass, prior to Pembrolizumab Therapy
Figure: Figure 2: Endoscopic Submucosal Dissection of Residual Colonic Mass. Image A, B – 3cm mass (Paris Classification mixed IIa + IIc) in forward view. C – Mass in retroflexed view. D – ESD of lesion. E – Post Resection Site. F – Resected Specimen
Disclosures: Anni Chowdhury Arellanes indicated no relevant financial relationships. Montserrat Guraieb Trueba indicated no relevant financial relationships. Van Karlyle II Morris indicated no relevant financial relationships. Phillip Ge: Aspero Medical – Consultant. Boston Scientific – Consultant. Fujifilm Medical Systems – Consultant. Neptune Medical – Consultant. Ovesco Endoscopy USA – Consultant. UpToDate – Royalties. Emmanuel Coronel indicated no relevant financial relationships.
Anni Chowdhury Arellanes, DO1, Montserrat Guraieb Trueba, MD1, Van Karlyle II Morris, MD1, Phillip S.. Ge, MD2, Emmanuel Coronel, MD2. P4630 - Endoscopic Submucosal Dissection of T3 MSI-high Colorectal Cancer Treated With Neoadjuvant Pembrolizumab, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.