Medical College of Georgia at Augusta University Augusta, GA
Anam Herekar, MD1, Karan Sharma, MS2, John N. McNally, DO1, Davis Hardell, 3, Rishik Marneni, 4, Stephen Schaffner, DO3, Amol Sharma, MD, MSc, FACG5 1Medical College of Georgia at Augusta University, Augusta, GA; 2Medical College of Georgia at Augusta University, Suwanee, GA; 3Augusta University Medical Center, Augusta, GA; 4University of Missouri - Kansas City School of Medicine, Kansas City, MO; 5Medical University of South Carolina, Charleston, SC Introduction: Annular Pancreas is an anatomical variant affecting approximately 3.4 per 100,000 individuals in United States in which the second part of the duodenum is either partially or fully encased by pancreatic tissue.1,2 This is caused by malrotation of ventral pancreatic bud during embryogenesis.2 Although most people are asymptomatic with this condition, complications arising from this include pancreatitis and duodenal obstruction. 2 Due to the scarcity of this condition in literature, we aimed to explore this further in an adult patient presenting to our hospital.
Case Description/
Methods: A 44-year-old female status-post laparoscopic cholecystectomy for suspected gallstone pancreatitis presented one-week post-op to an outside hospital due to persistent abdominal pain, nausea, and vomiting. Laboratory values at that time were notable for ALP 185 U/l, AST 37 U/l, ALT 73 U/l, and lipase 77 U/l. Computed tomography of abdomen/pelvis revealed partial high-grade duodenal obstruction resulting in dilated stomach and proximal duodenum secondary to annular pancreas; a new pancreatic tail lesion was also noted (Fig 1, 2). Esophagogastroduodenoscopy was performed and showed an acquired extrinsic severe duodenal obstruction. A nasogastric tube was placed on intermittent suction with partial symptomatic relief. The patient was then subsequently transferred to our tertiary care center for further evaluation and management. Upon additional review and questioning, she endorsed experiencing similar symptoms several years prior that self-resolved; however, she had never been previously diagnosed with a pancreatic pathology. Surgical gastrojejunostomy was soon thereafter performed, leading to a full resolution of the patient’s symptoms. Discussion: Annular pancreas is a rare congential anomaly that can cause duodenal obstruction in not only children but also adults as evident by our case. This case also highlights the importance of considering anatomical variants, such as annular pancreas, in the evaluation of patients with pancreatitis of unclear etiology. References 1. Alkhayyat M, Bachour S, Abou Saleh M, et al. The Epidemiology of Annular Pancreas in the United States: A Population-based Study. J Clin Gastroenterol. 2022 Feb 1;56(2):186-191. 2. Gromski MA, Lehman GA, Zyromski NJ, et al. Annular pancreas: endoscopic and pancreatographic findings from a tertiary referral ERCP center. Gastrointest Endosc. 2019 Feb;89(2):322-328.
Figure: Figure 1. Coronal plane of CT abdomen/pelvis revealing partial high-grade duodenal obstruction secondary to annular pancreas
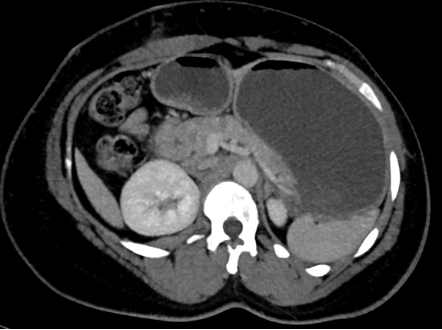
Figure: Figure 2. Axial plane of CT abdomen/pelvis revealing partial high-grade duodenal obstruction secondary to annular pancreas
Disclosures: Anam Herekar indicated no relevant financial relationships. Karan Sharma indicated no relevant financial relationships. John McNally indicated no relevant financial relationships. Davis Hardell indicated no relevant financial relationships. Rishik Marneni indicated no relevant financial relationships. Stephen Schaffner indicated no relevant financial relationships. Amol Sharma indicated no relevant financial relationships.
Anam Herekar, MD1, Karan Sharma, MS2, John N. McNally, DO1, Davis Hardell, 3, Rishik Marneni, 4, Stephen Schaffner, DO3, Amol Sharma, MD, MSc, FACG5. P4524 - Partial High Grade Duodenal Obstruction Due to Annular Pancreas in an Adult, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.