Mather Hospital, Northwell Health Port Jefferson, NY
Monica Arora, DO1, Tyler Santos, MD, MS1, Jaspreet Singh, MD2 1Mather Hospital, Northwell Health, Port Jefferson, NY; 2Northwell Health, Bay Shore, NY Introduction: Laparoscopic cholecystectomy (LC) is the gold standard for treating gallbladder disease, with approximately 750,000 procedures performed annually in the United States. LC carries a complication rate of about 3%, including bile leakage, stone recurrence, infection, bleeding, and, rarely, surgical clip migration. Surgical clip migration is an uncommon but clinically significant complication, with fewer than 100 cases reported in the literature. Migration can occur months to years postoperatively, with a median onset of approximately 26 months. Migrated clips have been found in various locations, including the common bile duct (CBD), duodenum, and even the pulmonary artery.
Case Description/
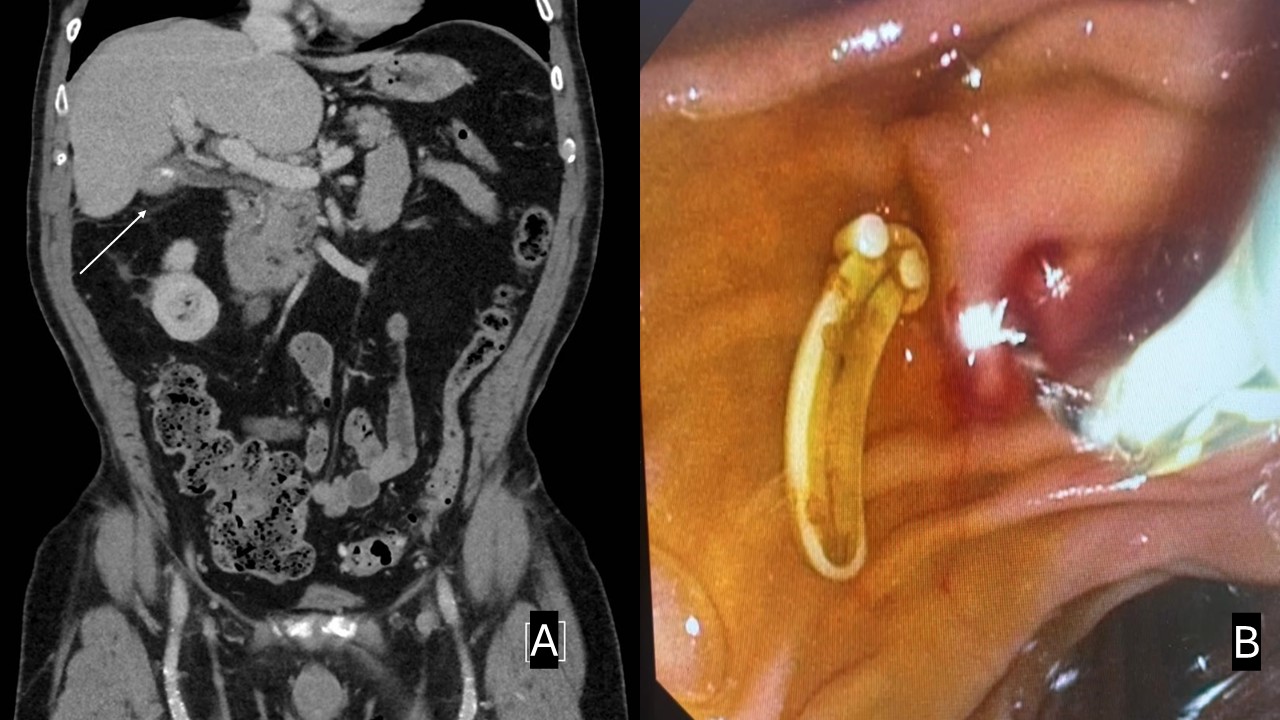
Methods: 74-year-old man who underwent laparoscopic cholecystectomy 5 months prior presents with persistent recurrent radiating right upper quadrant (RUQ) abdominal pain. Vital stable. Physical examination revealed tenderness in the RUQ. Unremarkable CBC and CMP with LFTs in the normal range. CT Abdomen and Pelvis showed bile ducts with punctate nonobstructive stones layering in the intrapancreatic portion of common bile ducts, cholecystectomy, an enhancing phlegmonous infiltration with scattered hypodensity gallbladder fossa adjacent to thickened cystic duct remnant and extending along Morison pouch and inferior liver tip to the right lateral peritoneal reflection (Figure A). No drainable collection was identified. Due to his ongoing symptoms, concern for biliary leak. Patient started antibiotics and underwent EGD/EUS/ERCP. EUS noted biliary sludge but no ductal dilation. CBD measured 6.2 mm. ERCP with sphincterotomy was then performed, which revealed biliary sludge and foreign body (consistent with cystic duct clip placed during cholecystectomy). It was removed from the bile duct using a 11.5 mm biliary stone extraction balloon (Figure B), resulting in the resolution of the patient’s symptoms. Discussion: This case underscores the diagnostic challenge posed by delayed-onset abdominal pain following LC. Migrated surgical clips, though rare, should also be considered, particularly in patients presenting with unexplained biliary symptoms. Risk factors for clip migration include acute cholecystitis at the time of surgery, excessive use of clips, and improper clip placement. The successful endoscopic removal of the migrated clip highlights the pivotal role of ERCP in managing this complication. Early recognition of clip migration can prevent further morbidity and facilitate timely intervention.
Figure: Figure A: CT Abdomen and Pelvis showed bile ducts with punctate nonobstructive stones layering in the intrapancreatic portion of common bile ducts, cholecystectomy, and an enhancing phlegmonous infiltration with scattered hypodensity gallbladder fossa adjacent to a thickened cystic duct remnant and phlegmonous infiltration extends along Morison pouch (white arrow) and inferior liver tip to the right lateral peritoneal reflection. Figure B: Removal of foreign body/ cystic duct clip from the common bile duct.
Disclosures: Monica Arora indicated no relevant financial relationships. Tyler Santos indicated no relevant financial relationships. Jaspreet Singh indicated no relevant financial relationships.
Monica Arora, DO1, Tyler Santos, MD, MS1, Jaspreet Singh, MD2. P4470 - Lost but Found: A Rare Case of Post-Cholecystectomy Clip Migration Presenting as Biliary Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.